Rhabdomyolysis is a serious medical condition that needs fast action and clear records. It happens when muscle tissue breaks down and releases harmful proteins into the blood. These proteins can damage the kidneys and cause life-threatening problems if care slows.
This condition often starts after trauma, extreme exercise, dehydration, or certain drugs. Patients may arrive weak, sore, confused, or unable to pass normal urine. Labs rise fast, hospital stays grow longer, and costs increase quickly.
That is why Rhabdomyolysis ICD 10 coding matters from the very first note. Accurate coding links medical care to correct payment and compliance.
This guide explains the codes, rules, and workflows in simple language.
Why Does Rhabdomyolysis ICD 10 Matter for Medical Billing?
Rhabdomyolysis often leads to hospital admission, repeat labs, IV fluids, and kidney monitoring. These services raise claim value and payer scrutiny. Clear documentation and accurate use of the rhabdomyolysis ICD 10 code help prove medical necessity, reduce denials, and speed reimbursement.
Rhabdomyolysis cases often lead to hospital admission. Many patients need close monitoring, fluids, and repeat lab testing. These services raise total charges very quickly.
Payers know this and review these claims with care. When coding lacks clarity, denials often follow. Revenue teams then spend weeks fixing avoidable issues.
Why does this condition impact revenue so much?
- Inpatient Stays Increase Overall Claim Value
- Kidney Injury Raises Risk for Dialysis Services
- Frequent Labs Trigger Payer Medical Reviews
What Is the Rhabdomyolysis ICD 10 Code?
The correct ICD 10 code for rhabdomyolysis is M62.82. Use this billable code only when a provider confirms muscle breakdown. Do not assign it based only on lab values. Sequence it first when rhabdomyolysis drives admission or treatment decisions.
The main code for this condition is easy to remember. The correct ICD 10 code for Rhabdomyolysis is M62.82. This code is billable and valid for reimbursement.
It applies when the provider clearly diagnoses rhabdomyolysis. Do not assign this code using labs alone. Elevated CK supports the diagnosis but does not replace provider wording.
2026 Coding Update Note
M62.82 remains a valid, billable ICD-10-CM code for rhabdomyolysis under the 2026 coding set (effective October 1, 2025). Always confirm the diagnosis is provider – documented before assignment and review annual updates for exclusions or sequencing rules.
Which ICD 10 Codes Are Used With Rhabdomyolysis?
Rhabdomyolysis rarely occurs alone. Coders must report related conditions such as acute kidney failure, dehydration, or trauma. Reporting all documented diagnoses strengthens medical necessity and protects higher-value inpatient claims from audits or denials.
Rhabdomyolysis often appears with other serious conditions. Coders must capture the full clinical picture accurately.
The table below lists the most common ICD 10 codes used with rhabdomyolysis and explains when each applies.
| ICD 10 Code | Description | When to Use | Clinical Indicators |
|---|---|---|---|
| M62.82 | Rhabdomyolysis | Confirmed muscle breakdown | CK levels > 5× normal, myoglobinuria, muscle pain |
| N17.9 | Acute kidney failure | Renal injury present | Rising creatinine, low urine output |
| E86.0 | Dehydration | Fluid loss documented | Dry mucosa, hypotension, elevated BUN |
| T79.6XXA | Traumatic muscle injury | Crush or trauma causes | Injury history, swelling, tissue damage |
| R74.8 | Abnormal CK | Labs abnormal only | Elevated CK without a confirmed diagnosis |
Use symptom codes only before diagnosis. Switch to Rhabdomyolysis ICD 10 once the provider confirms muscle breakdown. Secondary codes should always reflect conditions that affect treatment, monitoring, or length of stay.
Insight:
Accurate secondary coding shows severity, supports medical necessity, and protects Rhabdomyolysis ICD 10 claims during audits. When coders report all documented conditions, payers can clearly see why intensive care, frequent labs, or dialysis monitoring were required.
When Should You Use Rhabdomyolysis ICD 10 Instead of Symptoms?
This choice affects claim success and audit risk more than many teams expect. Rhabdomyolysis often starts with vague symptoms that look like common muscle strain or fatigue.
Coding too early or too late can weaken medical necessity and invite payer review. Symptoms alone never justify M62.82. Patients often present with muscle pain or weakness.
They may also show dark urine or abnormal labs. These signs suggest rhabdomyolysis but do not confirm it. Only the provider diagnosis allows use of the condition code.
What is the best way to code early encounters?
Start with symptom codes until the diagnosis becomes clear.
When should I stop using symptom codes?
When the provider documents rhabdomyolysis clearly in the assessment.
What Documentation Is Needed to Code Rhabdomyolysis?
Accurate coding depends on clear provider documentation. The record must confirm rhabdomyolysis, describe the cause, show lab trends, and outline treatment. Missing details weaken medical necessity and increase the risk of payer review or rejection.
Strong documentation protects both care quality and payment. Every chart must tell a clear story from start to finish. Providers should name the diagnosis directly. Supporting details must appear throughout the record.
Key documentation elements include:
- Clear Provider Diagnosis
- Creatine Kinase Levels and Trends
- Causes Such As Trauma, Drugs, Or Exertion
- Treatment Plan Including IV Fluids
- Kidney Monitoring and Consults
Missing details slow claims and raise audit risk because payers cannot confirm why high-cost care was needed. Incomplete records often lead to chart requests, delayed payments, downcoding, or full claim denials.
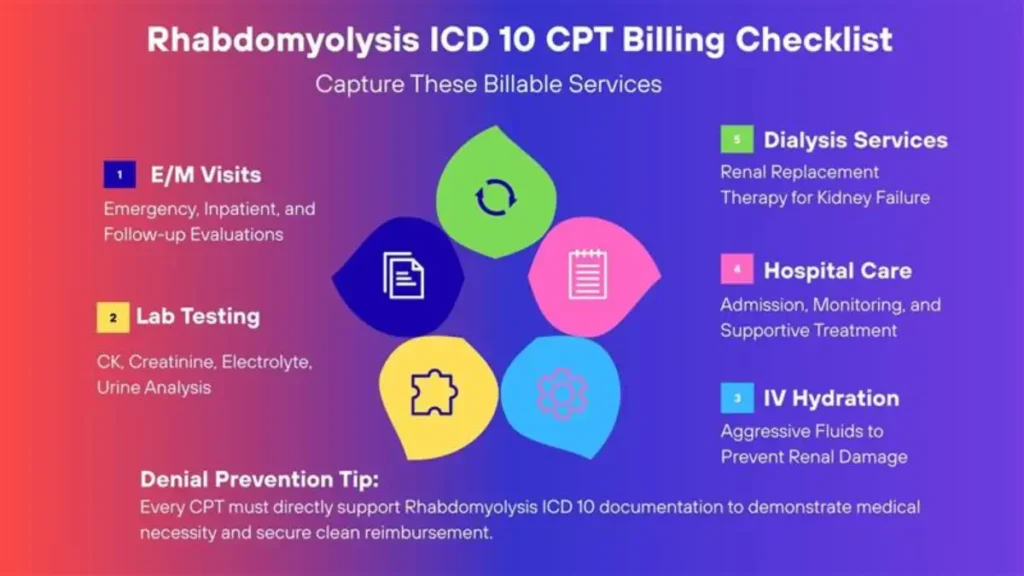
Which CPT Services Are Common in Rhabdomyolysis Cases?
Rhabdomyolysis care involves many billable services because patients often need urgent evaluation, aggressive fluids, and close kidney monitoring. Each service must connect clearly to the diagnosis to show why the care was medically necessary and appropriate for the patient’s condition.
Common CPT services include:
- Evaluation And Management Visits
- Blood And Urine Laboratory Testing
- IV Fluid Administration
- Inpatient Hospital Services
- Dialysis Support If Kidney Failure Occurs
Mismatch between CPT and diagnosis often causes denials because payers cannot see a clear reason for high-cost services. When procedures are not clearly supported by Rhabdomyolysis ICD 10, claims may face downcoding, payment delays, or full rejection.
How Do You Link Rhabdomyolysis ICD 10 to Procedures?
Every procedure needs medical justification. Diagnosis codes provide that support. Sequence Rhabdomyolysis ICD 10 first when it drives care. List related conditions after the primary diagnosis. Payers review this order closely. Incorrect sequencing can trigger edits or downcoding.
Payers evaluate medical necessity closely for rhabdomyolysis because treatment often includes high-cost services such as ICU monitoring, repeated labs, and dialysis.
Each CPT service must clearly connect to documented muscle breakdown, kidney risk, or fluid management. Claims without this link frequently trigger pre-payment review.
How did teams reduce denials?
By matching every CPT service to a documented clinical reason.
What Coding Errors Cause Rhabdomyolysis Claim Denials?
Most denials come from repeated mistakes because small documentation or coding gaps add up quickly. These errors are easy to avoid with care, clear workflows, and close review of the provider’s final assessment.
Common errors include:
- Coding Symptoms Instead Of Diagnosis
- Missing Provider Confirmation
- Using Unspecified Codes Unnecessarily
- Incorrect Diagnosis Sequencing
Each error weakens the claim’s credibility by breaking the link between the diagnosis and the care provided. When payers see inconsistencies, they question medical necessity and often delay, reduce, or deny payment.
How Do You Code Rhabdomyolysis Step by Step?
A clear workflow improves accuracy, speed, and claim confidence. Rhabdomyolysis cases move fast, and small errors can follow the claim for weeks. A simple, repeatable process helps teams apply Rhabdomyolysis ICD 10 correctly and avoid payer delays.
Step-by-step process:
- Review The Provider Assessment First
- Confirm Lab Results Support Documentation
- Assign ICD 10 for Rhabdomyolysis Only When Confirmed
- Add Related Condition Codes Carefully
- Validate CPT Alignment Before Submission
This process supports clean claims and faster payment by keeping diagnosis, labs, and services aligned. It also helps ensure Rhabdomyolysis ICD 10 reflects the true reason for care, not just abnormal test results.
Insight:
Consistent workflows lower rework and appeal rates because claims go out complete the first time. Teams that follow a standard process see fewer denials, faster reimbursement, and stronger audit outcomes.
How Does Accurate Rhabdomyolysis ICD 10 Coding Protect Revenue?
Because rhabdomyolysis claims involve high-cost care, payers review them closely. Correct sequencing, confirmed diagnoses, and complete documentation protect revenue. Clean claims pay faster and are less likely to face audits or post-payment recoupments.
Rhabdomyolysis claims attract audits due to the high cost. Payers expect strong documentation and correct coding. Accurate use of Rhabdomyolysis ICD 10 lowers risk. Clear records support medical necessity during reviews.
Why does accuracy matter so much?
Because clean claims pay faster and survive audits with ease.
Who Can Help You Code Rhabdomyolysis Correctly?
Rhabdomyolysis coding requires both clinical insight and billing skill. Small errors can lead to large financial losses.
Experienced partners help align documentation, coding, and compliance goals. They protect revenue while easing audit pressure.
This guide was reviewed by senior medical billing and coding specialists with over a decade of experience in inpatient hospital coding, denial prevention, and revenue cycle management.
Frequently Asked Questions
What is the specific ICD 10 code for rhabdomyolysis?
Assign M62.82 as the primary Rhabdomyolysis ICD 10 code for non-traumatic cases. This billable code identifies skeletal muscle breakdown. You must only use it when a provider explicitly confirms the diagnosis in the medical record. Never code based on elevated creatine kinase (CK) levels alone without a documented physician statement.
How do you code traumatic versus non-traumatic rhabdomyolysis?
The correct ICD 10 for rhabdomyolysis depends on the cause. Use M62.82 for exertional or drug-induced cases. For injuries like crush syndrome, use T79.6 (Traumatic ischemia of muscle). Misidentifying the etiology violates “Excludes1” rules and risks claim denials during payer audits for injury-related medical necessity.
Can you report an ICD 10 code for rhabdomyolysis based on high CK levels?
Official guidelines prohibit assigning an ICD 10 code for rhabdomyolysis using lab results alone. If the provider only notes “elevated CK,” use symptom code R74.8. You may only report M62.82 once the physician explicitly links those abnormal labs to a formal diagnosis of rhabdomyolysis in the assessment.
Which secondary codes should you link with ICD 10 rhabdomyolysis?
Link ICD 10 rhabdomyolysis with complications to support medical necessity. Frequently reported secondary codes include N17.9 (Acute kidney failure), E86.0 (Dehydration), and E87.5 (Hyperkalemia). Reporting these related conditions accurately reflects the patient’s severity of illness and justifies higher-level inpatient services or specialized monitoring during the hospital stay.
Why do payers frequently deny claims involving Rhabdomyolysis ICD 10?
Payers often deny claims when the Rhabdomyolysis ICD 10 code lacks a documented cause or clinical evidence. Denials also occur when the diagnosis does not match high-cost treatments like ICU monitoring or dialysis. Ensure the provider assessment bridges clinical indicators, like CK trends, directly to the final diagnosis.
