Cancer care is one of the most expensive, most closely watched corners of American healthcare, and the billing behind it reflects that. A single chemotherapy visit can involve a physician evaluation, an infusion service, multiple drug codes, wastage documentation, and a prior authorization that took two weeks to secure. Miss one detail and the claim comes back denied, sometimes months after the patient was treated.
If you work in an oncology practice, an infusion center, or a hospital-based cancer program, you already know this isn’t an exaggeration. Oncology Medical billing sits at the intersection of high-dollar drugs, tight payer rules, and documentation standards that leave almost no room for guesswork. This guide walks through how oncology billing actually works in 2026, the codes and modifiers that matter most, where claims break down, and what a practice can do to protect its revenue without slowing down patient care.
Why Oncology Medical Billing Is Different From Almost Every Other Specialty
Most specialties bill for a handful of predictable services. Oncology bills for an entire care pathway that changes from one visit to the next. A patient might receive an E/M visit, labs, imaging, a chemotherapy infusion, a supportive drug like an antiemetic, and a follow-up injection, all in the same encounter. Each of those pieces has its own code, its own documentation requirement, and its own payer rule.
A few things make oncology uniquely difficult to bill correctly:
- The drugs themselves are extraordinarily expensive, so payers scrutinize every unit billed. A rounding error on a HCPCS drug code can mean thousands of dollars in overpayment or underpayment.
- Treatment plans change based on how a patient responds, which means coding has to reflect what actually happened that day, not a fixed protocol.
- Almost every high-cost drug requires prior authorization, and oncology practices manage far more of these requests than the average specialty.
- Radiation oncology and medical oncology are billed completely differently, and a practice offering both needs staff who understand each pathway.
Because of all this, oncology claims are denied initially at a noticeably higher rate than general medical claims, and appeals eat up staff hours that could otherwise go toward clean claim submission in the first place.
Medical Oncology, Radiation Oncology, and Surgical Oncology: Three Different Billing Worlds
Before diving into codes, it helps to separate oncology billing into its three main branches, because payers treat them differently.
Medical oncology billing
Medical oncology billing covers chemotherapy, immunotherapy, targeted therapy, and biologic drug administration, along with the E/M visits and supportive care that surround them. This is where infusion coding, drug HCPCS codes, and administration hierarchies live.
Radiation oncology billing
Radiation oncology billing covers both the physician’s planning and management work and the technical delivery of radiation itself, whether that’s external beam therapy, brachytherapy, or stereotactic treatment. A single course of radiation can generate a dozen or more line items across simulation, planning, dosimetry, and daily treatment delivery, and each requires separate documentation.
Surgical oncology billing
Surgical oncology billing follows standard surgical coding rules but adds oncology-specific nuance around staging procedures, biopsies, and pathology coordination, since the surgical approach often depends on what the pathology report shows.
A practice that treats patients across all three pathways, such as a hospital-based cancer center, needs billing staff who can move between these worlds without mixing up the rules. This is one reason many organizations lean on staff with true specialty medical billing experience rather than general practice billers.
The Oncology Medical Billing Cycle, Step by Step
Oncology Medical billing follows the same broad revenue cycle as any specialty, but every step carries more weight because the dollar amounts are higher and the margin for error is smaller.
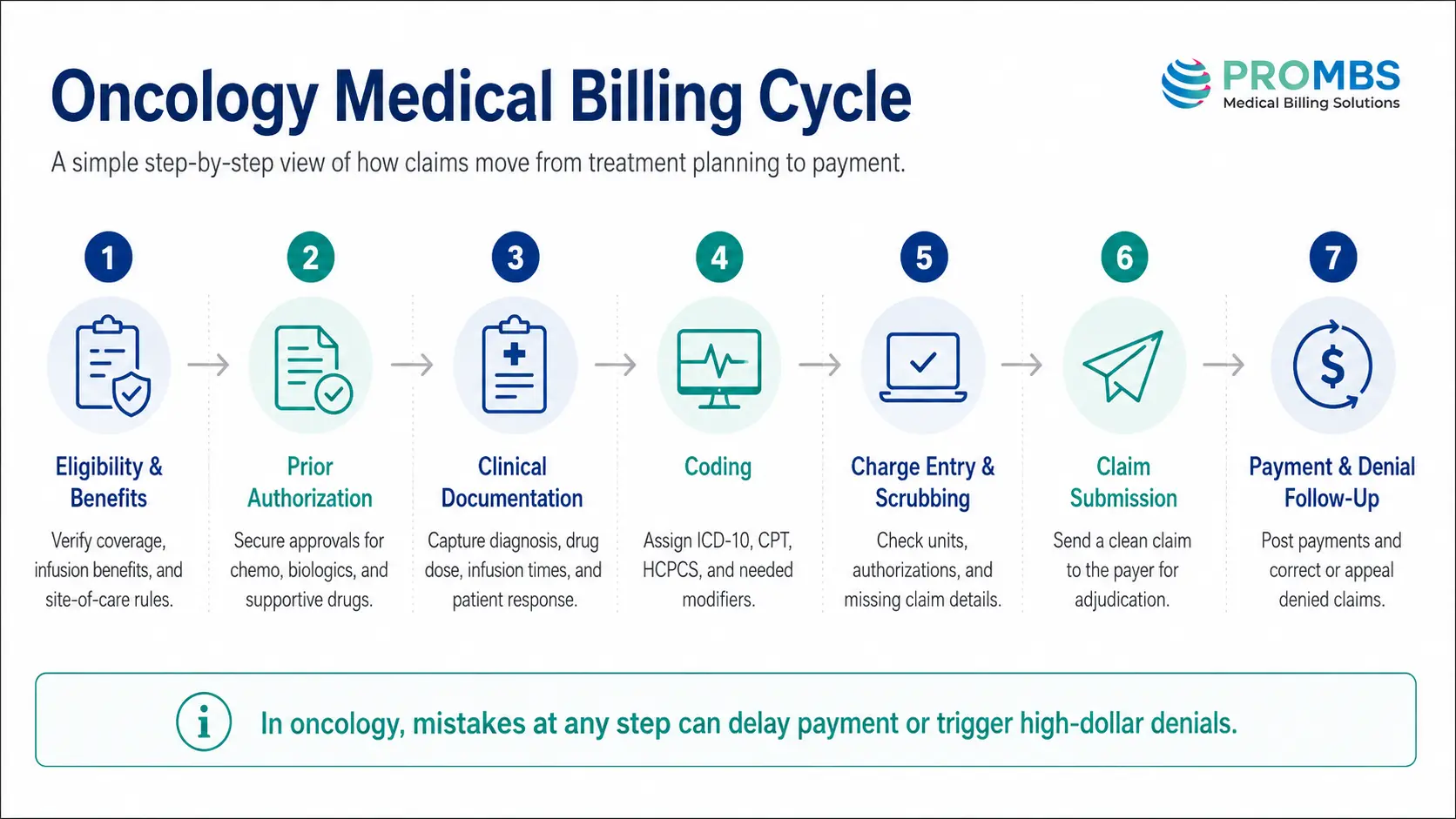
1. Eligibility and benefits verification
Before treatment starts, staff confirm the patient’s coverage for chemotherapy, radiation, and any specialty drugs planned. This step also identifies whether the payer requires site-of-care restrictions, meaning some plans will only reimburse infusions performed at specific facility types. Skipping or rushing this step is one of the fastest ways to end up with an unpaid claim, which is why a solid patient insurance verification process matters so much in oncology specifically.
2. Prior authorization
Nearly every chemotherapy regimen, biologic, and many supportive drugs require approval before the first dose. This step alone can take days to weeks and often needs to be repeated when a regimen changes.
3. Clinical documentation
Oncologists and nursing staff record the drugs administered, exact infusion start and stop times, dosages, and the patient’s response. This documentation is what coders rely on to assign accurate charges, and it’s also what supports the claim if the payer later requests records.
4. Coding
Coders translate the encounter into ICD-10 diagnosis codes, CPT administration codes, and HCPCS drug codes, applying the correct modifiers and sequencing rules.
5. Charge entry and claim scrubbing
Charges are entered into the billing system and passed through a scrubber that flags missing modifiers, mismatched units, or incomplete authorization data before the claim ever reaches the payer.
6. Submission and adjudication
Clean claims move to the payer for processing. In oncology, even a well-documented claim can trigger additional review simply because of the dollar value involved.
7. Payment posting and denial management
Payments are posted, and any denials are routed for correction or appeal. Given how often oncology claims come back with issues, this stage often needs a dedicated team rather than a generalist follow-up process.
CPT and HCPCS Codes Every Oncology Biller Needs to Know
Chemotherapy administration codes follow a hierarchy based on method and sequence, and getting this order wrong is one of the most common coding mistakes in oncology.
For intravenous push, the code depends on whether it’s the initial substance (96409) or a sequential push of a new drug (96411). For infusions, 96413 covers the initial IV infusion of a chemotherapy or biologic agent up to one hour, with an add-on code for each additional hour. When a second, different drug is infused sequentially through the same IV line, a separate sequential infusion code applies rather than billing it as a second initial infusion. Concurrent infusions, where two drugs run at the same time through the same line, have their own distinct code as well, and payers watch this hierarchy closely because billing multiple “initial” services on one encounter is a classic audit trigger.
Drug codes themselves are billed using HCPCS J-codes and Q-codes, each representing a specific drug and dosage unit. The billed units must match exactly what was administered, including any documented waste, and coders need to keep these code sets current since new drugs and biosimilars are added regularly.
E/M visits billed alongside a procedure on the same day typically need modifier 25 attached to show the visit was a separately identifiable service from the treatment itself. Getting this modifier wrong, either by overusing it or leaving it off when it’s needed, is one of the most frequent reasons E/M charges get denied in oncology. If your team wants a deeper refresher on when this modifier does and doesn’t apply, this guide to modifier 25 in medical billing breaks it down clearly, and this broader piece on what a modifier actually does in medical billing is a useful primer for newer staff.
Radiation oncology uses its own separate code families for simulation, treatment planning, dosimetry, and daily treatment delivery, and hospital-based programs also need to separate professional charges from technical facility charges, which are billed under entirely different rules.
ICD-10 Coding for Cancer Diagnoses
Oncology ICD-10 coding is unusually specific. Malignant neoplasm codes are built around the exact site of the primary tumor, whether the cancer is primary or secondary (metastatic), and the patient’s current treatment status. A code for active breast cancer looks nothing like the code used once that same patient is in remission and being monitored, which falls under personal history of malignant neoplasm codes instead.
This distinction matters enormously for reimbursement. Billing an active cancer code for a patient who has completed treatment and is now in surveillance can trigger a payer audit, while using a history code too early can cause a legitimate treatment claim to be denied for lack of medical necessity. Coders need to cross-check the diagnosis code against the treatment note every single time rather than defaulting to whatever code was used on the last visit.
Secondary or metastatic disease also needs its own set of codes reflecting the site of metastasis, and both the primary and secondary sites usually need to be reported together to fully justify the treatment plan on the claim.
Drug Wastage: The JW and JZ Modifier Rules
This is one area where a lot of general billing guides fall short, and it’s worth understanding well because CMS made it a hard requirement rather than a suggestion. When a single-dose vial contains more medication than a patient needs, the unused, discarded portion can still be billed, but only if it’s properly documented and reported with modifier JW. Since mid-2023, CMS also requires modifier JZ on claims where there was no discarded drug at all, confirming that the full vial was administered.
This means every single-dose drug claim now needs one of these two modifiers present, and leaving both off is treated as an incomplete claim by many payers. Practices that don’t track wastage carefully tend to lose money in one of two ways: they either fail to bill for legitimate waste they’re entitled to, or they get flagged in an audit for reporting waste without adequate nursing documentation to support it. A simple internal policy requiring nurses to log vial size, dose administered, and amount wasted on every infusion note closes this gap quickly.
Watching your oncology claims get stuck on drug units, wastage documentation, or prior authorization?
ProMBS works with oncology practices and infusion centers to clean up coding, tighten documentation, and get claims paid faster the first time.
Buy and Bill, White Bagging, and Biosimilar Complications
Most oncology drugs are handled under a buy-and-bill model, where the practice purchases the drug, administers it, and then bills the payer for reimbursement. This puts real financial risk on the practice, since a denied or underpaid claim means absorbing the cost of an expensive drug that’s already been used.
An increasing number of payers are pushing practices toward white bagging instead, where a specialty pharmacy ships the drug directly to the practice for a specific patient, or brown bagging, where the patient picks up the drug and brings it to their appointment. Both models shift financial risk away from the practice but introduce their own headaches, including drug handling delays, waste that can’t be billed the same way, and the risk of a canceled appointment leaving an unusable, patient-specific drug on the shelf.
Biosimilars add another layer. Each biosimilar has its own distinct Q-code, separate from the reference biologic, and payers frequently have their own preferred product lists. Billing the wrong Q-code for a biosimilar, even one that’s clinically equivalent to another product, will result in a denial, so coders need to verify the exact product administered against the exact code billed rather than assuming interchangeability.
Prior Authorization: Oncology's Biggest Bottleneck
Prior authorization is consistently the single biggest administrative burden in oncology medical billing. Chemotherapy regimens, biologics, targeted therapies, and even some supportive drugs almost always require approval before the first dose, and any change in regimen, dose, or drug typically triggers a new request. Oncology practices routinely handle dozens of these requests every week, and staff can easily lose the better part of a workday just managing the paperwork and follow-up calls involved.
The financial risk here is significant because treatment usually can’t wait for a slow approval, which pushes some practices to start care before authorization is finalized. When that happens and the request is later denied, the practice can be left absorbing the full cost of an expensive round of treatment.
The most effective defense is a standing operating procedure that flags every drug requiring authorization before it’s ever ordered, tracks each request’s status daily, and assigns a specific staff member to own follow-up rather than letting requests sit in a shared inbox. If your team is still building this workflow, this resource on prior authorization as a revenue bottleneck and this one on cutting prior authorization denials both offer practical starting points.
Why Oncology Claims Get Denied, and How to Fix Each Cause
Oncology denial patterns tend to repeat themselves, which means most of them are preventable with the right process in place.
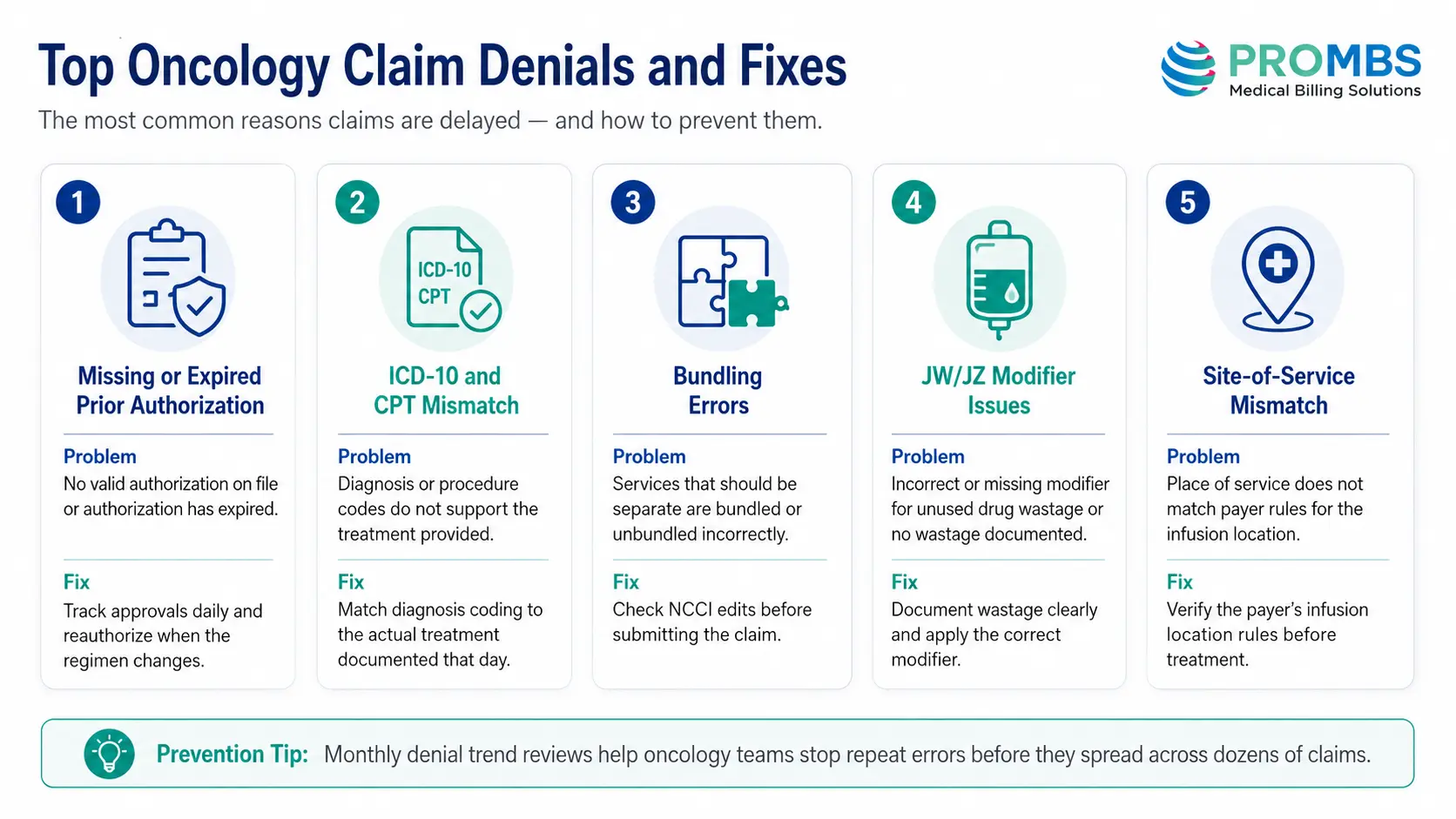
Missing or expired prior authorization
Missing or expired prior authorization is the single most common cause. The fix is a tracking system that flags authorizations before they expire and before a regimen change invalidates the existing approval.
ICD-10 and CPT mismatch
ICD-10 and CPT mismatch, where the diagnosis code doesn’t clearly support the treatment billed, is another frequent trigger. This overlaps heavily with what payers code as a CO-11 denial, and understanding why CO-11 denials for CPT mismatches keep happening can help staff catch this before submission rather than after.
Bundling errors
Bundling errors, where separately billable services get denied because they overlap with another code on the same claim, often trace back to National Correct Coding Initiative edits. Staying current with these rules through a resource like this NCCI edits and MUE update guide helps coders catch conflicts before they become denials.
Wastage documentation gaps
Wastage documentation gaps, tied to the JW and JZ modifier requirements covered earlier, are increasingly common now that payers actively audit for missing modifiers.
Site-of-service mismatches
Site-of-service mismatches, where a payer’s plan restricts infusion services to a specific facility type, catch practices off guard when a patient’s plan changes mid-treatment without anyone verifying it. Building a habit of re-checking eligibility at every new authorization cycle, not just at intake, closes this gap.
Clinical Trials and Research Billing
Oncology practices involved in clinical trials face an additional layer of complexity, since services need to be split between what’s covered by the study sponsor and what’s billed to the patient’s insurance as routine care. Medicare and most commercial payers will cover routine costs associated with a qualifying clinical trial, meaning the standard care a patient would have received anyway, but they won’t cover the experimental intervention itself or any service the trial protocol is specifically paying for.
Getting this split wrong in either direction creates problems. Billing the payer for something the sponsor should be covering is considered a compliance violation, while failing to bill the payer for legitimately covered routine costs leaves reimbursement on the table. Practices running trials need a dedicated research billing coordinator who cross-references every claim against the trial’s coverage analysis before it goes out.
Compliance and Audit Risk
Because oncology claims involve such high dollar amounts, payers and auditors pay closer attention to this specialty than almost any other. Common audit triggers include inconsistent drug units relative to documented dosage, missing JW or JZ modifiers, E/M visits billed with modifier 25 on a high percentage of encounters, and diagnosis codes that don’t clearly evolve as a patient’s treatment status changes over time.
Building compliance into the workflow rather than treating it as a once-a-year audit exercise makes the biggest difference. That means routine internal chart-to-claim reviews, a documented policy for wastage reporting, and regular staff training whenever CPT, HCPCS, or payer policy updates are released. A broader medical billing and coding compliance framework gives a useful structure for building this kind of ongoing review process, and running periodic checks against a medical billing audit checklist helps catch problems before a payer does.
Key Metrics to Track in Oncology Revenue Cycle Management
A handful of numbers tell you whether your oncology medical billing process is actually working.
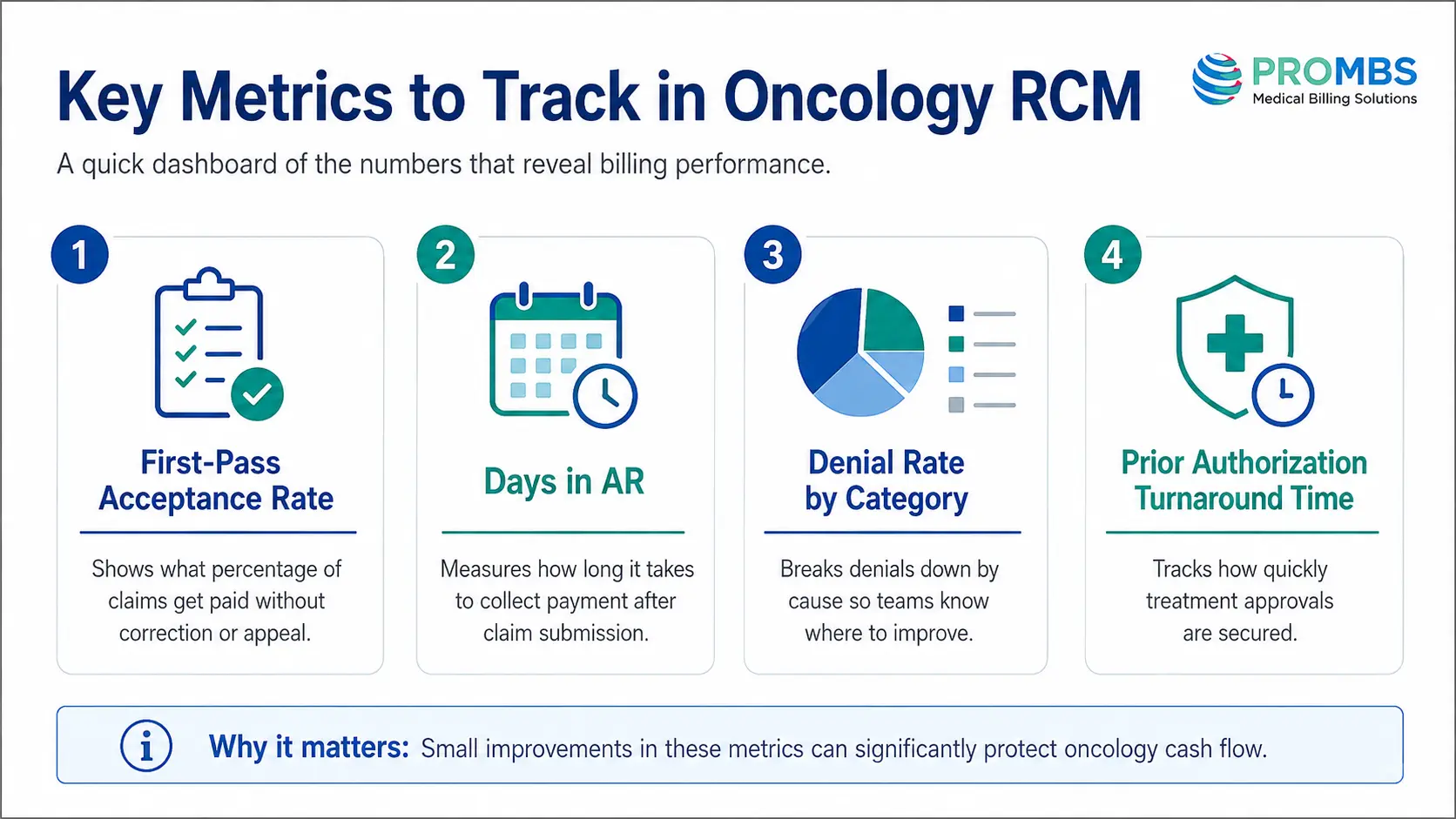
- First-pass acceptance rate shows what percentage of claims get paid without needing correction or appeal. Given how complex oncology claims are, even a modest improvement here has an outsized impact on cash flow.
- Days in accounts receivable measures how long it takes to collect payment after a claim is submitted. Oncology practices tend to run higher than average here because of appeal timelines, so tracking this by payer helps identify which relationships need attention.
- Denial rate by category breaks denials down by cause, whether that’s prior authorization, coding mismatch, or documentation, so leadership can see exactly where to focus process improvements rather than guessing.
- Prior authorization turnaround time tracks how long it takes from request to approval, which directly affects how quickly treatment can start and how much financial exposure the practice carries in the meantime.
For a broader look at how these figures connect to overall financial health, this guide on revenue cycle KPIs and this overview of receivable management in healthcare are worth reviewing alongside your own numbers.
A Practical Checklist to Strengthen Oncology Medical Billing
- Verify eligibility and site-of-service restrictions before every new treatment cycle, not just at initial intake.
- Confirm prior authorization status before each infusion, and flag any regimen change immediately for reauthorization.
- Require nursing documentation to include exact infusion start and stop times, vial size, dose given, and any wasted amount on every single encounter.
- Apply JW or JZ modifiers on every single-dose drug claim without exception.
- Double-check that the ICD-10 diagnosis code reflects the patient’s current treatment status, not a carried-over code from a prior visit.
- Run every claim through a scrubber that checks CPT and HCPCS pairing, modifier use, and NCCI bundling edits before submission.
- Review denial trends monthly by category so the same mistake doesn’t repeat across dozens of claims before anyone notices.
- Keep coders and billers current on CPT, HCPCS, and payer-specific oncology policy changes, since these shift more often in oncology than in most specialties.
In-House Oncology Billing vs Outsourcing
Some larger oncology groups keep billing in-house because it allows tighter coordination between clinical and billing staff, particularly for prior authorization and documentation review. The tradeoff is the ongoing cost of training and retaining staff who understand oncology-specific coding, which is a narrower skill set than general medical billing.
Smaller practices and infusion centers more often lean toward outsourcing to a billing partner with dedicated oncology experience, since the complexity of chemotherapy sequencing, drug wastage rules, and prior authorization volume can overwhelm a generalist team quickly. Neither path is automatically right for every practice, and the decision usually comes down to volume, staff expertise, and how much bandwidth clinical leadership has to oversee the revenue cycle directly. This comparison of outsourced medical billing versus in-house teams walks through the tradeoffs in more depth if your practice is weighing this decision.
Not sure whether your oncology billing should stay in-house or move to a specialized partner?
ProMBS reviews your current denial patterns, prior authorization workflow, and coding accuracy at no cost and shows you exactly where revenue is slipping through.
Frequently Asked Questions
What's the difference between medical oncology billing and radiation oncology billing?
Medical oncology billing covers chemotherapy, immunotherapy, and drug administration, while radiation oncology billing covers physician planning and the technical delivery of radiation treatment. They use entirely separate code sets and are usually handled by billers with different specialty training.
9. Denial ManagemenWhy do oncology claims get denied so often?t and Root-Cause Correction
The most common causes are missing or expired prior authorization, mismatched ICD-10 and CPT codes, incomplete infusion documentation, and missing JW or JZ wastage modifiers. Most of these are preventable with a consistent pre-submission review process.
Do all chemotherapy drugs require prior authorization?
Nearly all chemotherapy, biologic, and targeted therapy drugs require prior authorization from commercial payers, and many supportive drugs do as well. Requirements vary by payer and plan, so eligibility should be checked at the start of every new treatment cycle.
What is the JW modifier used for in oncology billing?
The JW modifier reports the amount of a single-dose drug that was discarded rather than administered to the patient, allowing that wasted portion to still be billed when properly documented. The JZ modifier, required since 2023, confirms that no drug was wasted at all.
Should a small oncology practice handle billing in-house or outsource it?
It depends on claim volume and staff expertise. Practices without dedicated, oncology-trained billing staff often find that outsourcing reduces denials and speeds up payment, while larger groups with experienced in-house teams may prefer to keep the process internal for tighter clinical coordination.
Final Thoughts
Oncology medical billing rewards precision more than almost any other specialty. The drugs are expensive, the documentation standards are strict, and payers scrutinize every claim closely, which means small process gaps compound into real revenue loss over time. Practices that build strong habits around prior authorization tracking, accurate wastage reporting, and clean chart-to-claim documentation consistently see fewer denials and faster payment, regardless of whether they manage billing internally or through a specialized partner.
Getting this right isn’t about adding more staff or more software. It’s about building a workflow where every claim is checked against the same standard before it ever reaches a payer.
