Tick bites are more than just a nuisance, they carry significant clinical and billing implications. Providers often encounter patients with tick bites presenting for wound care, tick removal, or concerns about infections such as Lyme disease, ehrlichiosis, or Rocky Mountain spotted fever. From a coding perspective, accurately applying the ICD 10 code for tick bite is essential for claim approval, correct reimbursement, and avoiding compliance pitfalls.
In medical billing, specificity matters. Whether the tick bite is on the arm, leg, torso, or scalp, coders must document and assign the correct ICD-10-CM code that reflects both the encounter type and anatomical location. Missteps, such as using an unspecified code when a more detailed option is available, often lead to denials.
This guide covers the ICD 10 code for tick bite, documentation requirements, billing workflow, and coding guidelines to help practices achieve cleaner claims and faster reimbursement.
What is Tick Removal?
Tick removal refers to the clinical procedure of extracting the tick from the patient’s skin using sterile techniques. Depending on severity, removal can be done with fine-tipped forceps in the office setting or may require minor surgical intervention if the mouthparts remain embedded.
From a billing perspective, coders must differentiate between evaluation and management (E/M) visits where tick removal is incidental versus procedural coding where removal involves complexity. Correct linkage between the ICD 10 code for tick bite and any CPT code for tick removal ensures accurate payer adjudication.
ICD 10 Codes for Tick Bite (2025 Updates)
The ICD 10 code for tick bite falls under the injury and external cause category. Coders must pay attention to site-specific codes and encounter types:
ICD-10 Codes for Tick Bite (Nonvenomous Insect Bite by Location)
| ICD-10 Code | Description |
|---|---|
| S30.861A | Insect bite (nonvenomous) of abdomen, initial encounter |
| S40.861A | Insect bite (nonvenomous) of upper arm, initial encounter |
| S70.361A | Insect bite (nonvenomous) of thigh, initial encounter |
| S80.861A | Insect bite (nonvenomous) of lower leg, initial encounter |
| S00.86XA | Insect bite (nonvenomous) of scalp, initial encounter |
Since ICD-10-CM does not list a unique code for “tick bite,” providers must code it under insect bite (nonvenomous) for the correct body site. If infection follows (e.g., cellulitis, Lyme disease), an additional diagnosis code should be assigned.
When documenting:
- A = initial encounter (active treatment such as tick removal)
- D = subsequent encounter (follow-up care, wound checks)
- S = sequela (late effects such as scarring or secondary infections)
Using the correct 7th character is crucial for payer compliance.
How to Bill for Tick Removal Procedures
Common CPT Codes for Tick Removal
10120 – Incision and removal of foreign body, subcutaneous tissues
Often used when a tick’s head or mouthparts remain embedded and require a minor surgical incision for removal.
99201–99215 – Evaluation and Management (E/M) office visits
Applied when tick removal is performed without incision, usually with forceps or other non-invasive techniques. The selection of the specific E/M level depends on the complexity of the visit and documentation of medical decision-making.
Key Steps for Proper Billing
1- Thorough Documentation
The provider’s note should clearly state:
The location of the tick bite (e.g., upper arm, scalp, thigh)
Whether removal was simple or required incision
The method used (manual extraction vs. surgical removal)
Any complications such as retained parts or infection
This documentation justifies both the ICD 10 code for tick bite and the procedural code.
2- Correct CPT–ICD-10 Linkage
Always link the tick bite diagnosis code with the procedure code used. For example:
CPT 10120 + ICD-10 S40.861A → incision and removal of tick bite from the upper arm, initial encounter.
CPT 99213 + ICD-10 S00.86XA → E/M office visit for removal of tick from the scalp, initial encounter.
This linkage demonstrates medical necessity and ensures payer systems recognize the claim as valid.
3- Modifier Usage When Applicable
Modifier -25: Append to an E/M code when the provider performs a significant, separately identifiable E/M service on the same day as the tick removal. Example: if the provider also evaluates the patient for Lyme disease risk or prescribes prophylactic antibiotics, the E/M visit is above and beyond the procedure.
Modifier -59: Occasionally required if tick removal is billed with other minor procedures to indicate distinct procedural services.
Billing Workflow Example
Imagine a patient presents with a tick embedded in the lower leg:
Provider performs an incision to fully remove the tick → CPT 10120
ICD-10 diagnosis: S80.861A – Insect bite (nonvenomous) of lower leg, initial encounter
If provider also conducts a detailed assessment for infection risk → CPT 99213-25 may be added.
This correct coding sequence ensures the claim is paid in full without delays.
Tick Removal Coding and Billing Guidelines
Accurate tick removal billing goes beyond simply selecting a code, it requires aligning documentation, ICD-10 diagnosis coding, CPT procedure coding, and payer-specific rules. By following structured guidelines, coders can reduce denials, improve claim approval rates, and maintain compliance.
1. Documentation Requirements
Strong documentation is the backbone of medical billing. Without it, even the correct ICD 10 code for tick bite or CPT code may be denied. The provider’s note should include:
Anatomical location of the bite – Site-specific codes (arm, leg, scalp, etc.) must match the documented location.
Encounter type – Initial (A), subsequent (D), or sequela (S). For example, S40.861A for initial removal versus S40.861D
for follow-up wound check.
Removal method – Whether the tick was extracted manually with forceps or required incision (CPT 10120). This establishes medical necessity.
Complications – Secondary infection, retained mouthparts, or systemic symptoms should be clearly stated, since they may justify additional ICD-10 codes.
2. Code Sequencing
Claims must be sequenced correctly to reflect clinical reality:
Primary diagnosis: The specific ICD 10 code for tick bite based on site and encounter type.
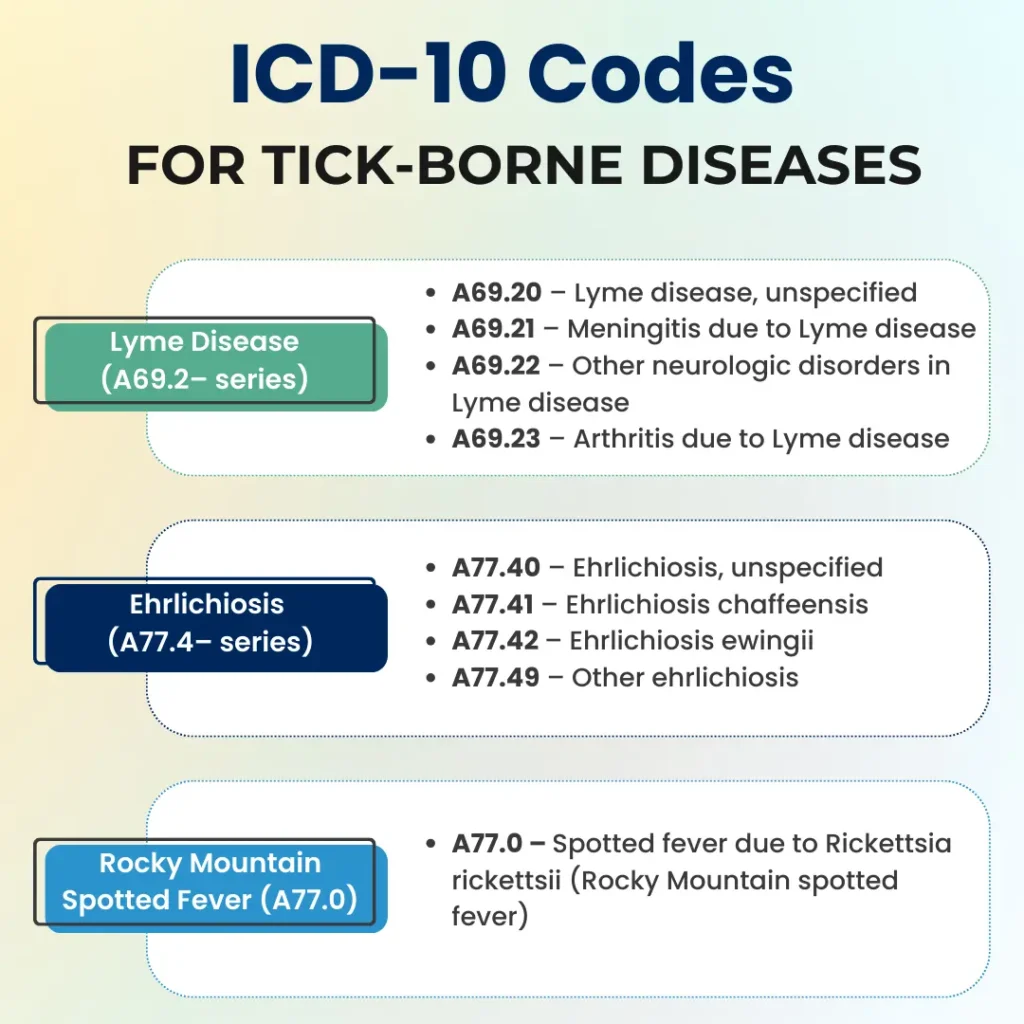
Secondary diagnosis: Any related condition, such as:
- B88.2 – Lyme disease carrier
- A77.0 – Rocky Mountain spotted fever
- L03.115 – Cellulitis of lower limb (if infection develops at the site)
- W57.XXXA – Bitten or stung by nonvenomous insect, initial encounter (external cause code if required by payer)
Correct sequencing ensures the payer understands the relationship between the tick bite and subsequent conditions.
3. CPT/ICD Linkage
Linkage between ICD-10-CM diagnosis codes and CPT procedure codes is mandatory for payer acceptance. Examples include:
CPT 10120 + S80.861A → Incision and removal of tick from lower leg, initial encounter.
CPT 99213 + S00.86XA → Office visit for tick bite on scalp, initial encounter, removed without incision.
If linkage is missing or inconsistent, payers may deny the claim citing “lack of medical necessity.”
4. Payer-Specific Nuances
Different payers have unique rules coders must respect:
Modifier -25 – Required by Medicare and many commercial payers when an E/M service is billed on the same day as
a tick removal procedure. Without it, the E/M charge will likely be denied.
Z20.828 – Some insurers request the use of this code (Contact with and suspected exposure to other communicable diseases) when Lyme disease testing is performed after a tick bite. This shows why the lab test was ordered.
Medicaid programs – May have stricter rules on when CPT 10120 is justified versus billing an E/M only. Always verify state-specific billing guidance.
5. Avoiding Denials
Common denial triggers in tick removal billing include:
Unspecified site coding – Using general insect bite codes when a specific anatomical code exists (S40.861A vs. unspecified bite).
Improper CPT/E/M pairing – Billing both an E/M visit and tick removal CPT without documentation of a distinct, medically necessary evaluation.
Missing 7th character – Leaving out “A,” “D,” or “S” at the end of the ICD-10 code, which makes the diagnosis incomplete.
Incomplete documentation – Not specifying whether the tick was superficial or required incision.
By proactively addressing these issues, practices can improve their first-pass claim acceptance rate and minimize costly rework.
Conclusion
Correctly applying the ICD 10 code for tick bite is essential for accurate billing, clean claims, and timely reimbursement. Since tick bites fall under nonvenomous insect bites, coders must select the site-specific ICD-10-CM code, ensure correct encounter character, and link the diagnosis with the appropriate CPT removal or E/M service.
Inaccurate coding leads to denials, delayed payments, and compliance risks. By following tick removal documentation requirements, payer-specific guidelines, and proper sequencing, providers can achieve optimal reimbursement.
For healthcare practices dealing with tick bite cases, mastering these coding rules not only prevents denials but also strengthens revenue cycle performance. Accurate use of the ICD 10 code for tick bite ensures both clinical integrity and financial efficiency.



