Quick Summary:
The primary ICD-10-CM code for carpal tunnel syndrome is G56.0, with specific codes indicating the side affected: G56.01 (right upper limb), G56.02 (left upper limb), and G56.03 (bilateral). These codes are used to diagnose median nerve compression causing hand numbness, pain, and tingling.
Key ICD-10-CM Codes for Carpal Tunnel Syndrome
- 00: Carpal tunnel syndrome, unspecified upper limb
- 01: Carpal tunnel syndrome, right upper limb
- 02: Carpal tunnel syndrome, left upper limb
- 03: Carpal tunnel syndrome, bilateral
Common Causes and Symptoms
Carpal tunnel syndrome involves pressure on the median nerve in the wrist, often caused by:
- Repetitive wrist motion
- Wrist injuries
- Rheumatoid arthritis or other underlying conditions
- Symptoms include burning pain, numbness, tingling, and difficulty grasping objects.
Introduction
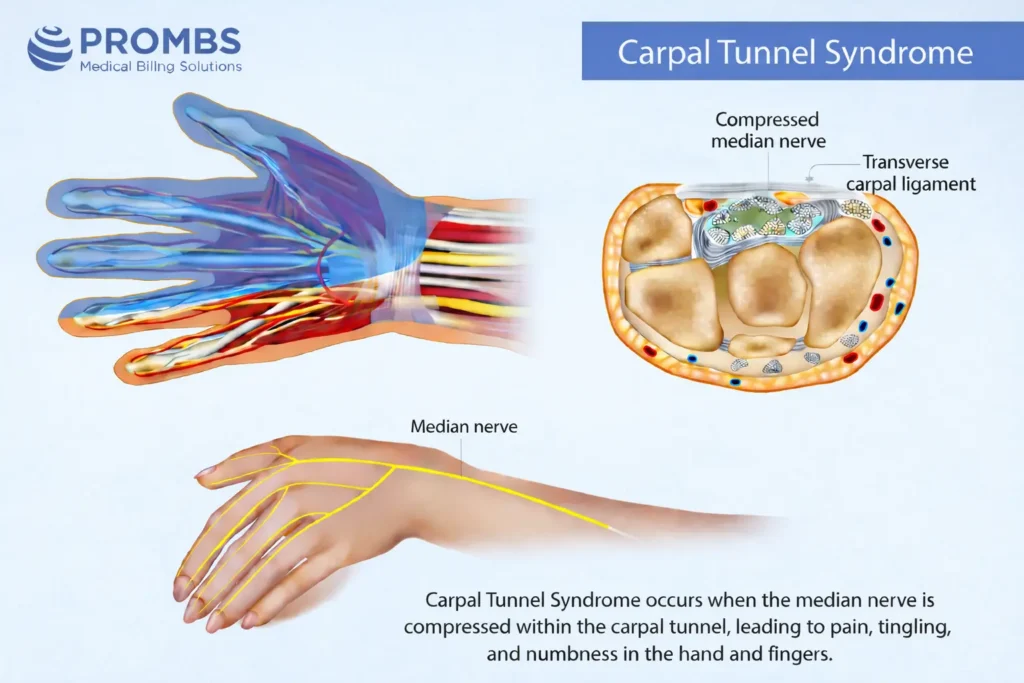
Carpal Tunnel Syndrome (CTS) occurs when the median nerve in your wrist becomes compressed. This often happens due to repetitive hand movements or chronic inflammation. According to the National Institute of Neurological Disorders and Stroke (NINDS), it remains one of the most frequent work-related conditions in the U.S.
When a patient experiences numbness, tingling, or weakness in their hand, doctors typically recommend treatments like:
- Nerve conduction testing
- Wrist splinting
- Steroid injections
- Surgical release
From a medical billing perspective, using the correct carpal tunnel syndrome ICD 10 code is about more than just paperwork - it’s about proving "medical necessity."
Insurance payers and CMS (Centers for Medicare & Medicaid Services) closely monitor these claims. If a medical record only mentions "hand pain" instead of using a specific ICD 10 for carpal tunnel syndrome, the claim might be denied.
As of 2026, the American Health Information Management Association (AHIMA) continues to stress that vague descriptions lead to "unspecified" codes. To ensure clean claim submissions and protect a practice's revenue, providers must use the specific ICD 10 carpal tunnel syndrome codes that identify exactly which hand is affected.
Symptoms of Carpal Tunnel Syndrome for Coders to Recognize
In clinical settings, carpal tunnel syndrome ICD 10 codes are justified by specific physical findings. Most patients describe a combination of pain, numbness, and "pins and needles" (paresthesia) in the thumb, index, and middle fingers.
According to the Mayo Clinic, these symptoms often spike at night or during repetitive hand tasks. For a coder, these details aren’t just medical notes - they are the evidence needed to justify diagnostic tests like Nerve Conduction Velocity (NCV) studies or surgical procedures.
2026 Documentation & Billing Requirements
To support the ICD 10 for carpal tunnel syndrome, provider notes must be explicit. Avoid vague terms like "hand pain" and instead look for "median nerve entrapment" or "nerve compression at the wrist."
| Clinical Indicator | Documentation Requirement | Billing Value (2026 Standards) |
|---|---|---|
| Numbness in first 3 fingers | Note if the symptoms are in the right, left, or both hands. | Required for laterality in ICD 10 carpal tunnel syndrome codes. |
| Positive Phalen’s Test | Document the physical exam maneuver used to confirm compression. | Supports medical necessity for NCV testing (CPT 95910). |
| Muscle Weakness | Detail any loss of grip strength or visible muscle wasting. | Justifies the transition from therapy to surgical intervention. |
| Nocturnal Pain | Record if pain worsens at night or during specific work activities. | Helps link the diagnosis to repetitive-strain classifications. |
Why Accuracy Matters
When the documentation is this clear, it creates a transparent trail for payers. It allows you to confidently assign the specific carpal tunnel syndrome ICD 10 code (G56.01, G56.02, or G56.03) and avoid the "unspecified" codes that trigger audits.
Did You Know?
The CDC reports that over 500,000 carpal tunnel surgeries are performed annually in the U.S. This makes it one of the most frequently billed nerve conditions in outpatient care today.
What Is the Specific ICD 10 Code for Carpal Tunnel Syndrome?
In the ICD-10-CM system, carpal tunnel syndrome falls under Chapter VI: Diseases of the Nervous System (G00–G99). The base code is G56.0, which specifically identifies median nerve compression at the wrist.
To meet 2026 billing standards, you must expand this code to the 5th digit to specify which hand is affected:
- 01: Carpal tunnel syndrome, right side
- 02: Carpal tunnel syndrome, left side
- 03: Carpal tunnel syndrome, bilateral (both sides)
Why Laterality is the Key to Reimbursement
Payers like CMS and Blue Cross Blue Shield now strictly require these specific codes. If a provider documents "bilateral CTS," using anything other than G56.03 could lead to a denial. Clear coding is especially vital when a patient undergoes surgery or nerve studies on both hands, as the code must justify the use of bilateral modifiers.
| ICD-10 Code | Description | Use Case & Coverage Logic |
|---|---|---|
| G56.00 | Unspecified side | Avoid this. Only use if the side is truly unknown, as it often triggers audits. |
| G56.01 | Right side | Use when symptoms and NCV tests confirm right median nerve involvement. |
| G56.02 | Left side | Use when clinical findings confirm left wrist nerve compression. |
| G56.03 | Bilateral | Supports "both hands" and justifies bilateral CPT modifiers (like -50). |
Protecting Your Practice from Audits
Precision in your ICD 10 carpal tunnel syndrome selection isn't just about getting paid - it's about staying compliant. The Office of Inspector General (OIG) has found that nearly 18% of denied hand-surgery claims were the result of mismatched laterality (for example, coding for the left hand when the notes described the right).
By correctly assigning the ICD 10 for carpal tunnel syndrome based on the specific hand affected, you create a clear clinical trail that satisfies both medical and insurance requirements.
Which CPT Codes Pair with the ICD 10 Code for Carpal Tunnel Syndrome?
The American Medical Association (AMA) categorizes carpal tunnel procedures into two main groups: diagnostic testing and surgical intervention. To receive reimbursement, each of these CPT codes must be linked to a specific ICD 10 for carpal tunnel syndrome (G56.01, G56.02, or G56.03).
Common CPT and ICD-10 Pairings for 2026
| CPT Code | Procedure Description | Medical Necessity Support |
|---|---|---|
| 95910 | Nerve conduction study | Requires documented clinical suspicion of median neuropathy. |
| 95886 | Needle electromyography (EMG) | Must reference EMG findings that confirm CTS under AANEM standards. |
| 64721 | Carpal tunnel release (Surgery) | Justified when conservative treatments (like splinting) have failed. |
| 20526 | Therapeutic injection | Requires a pre-procedure diagnosis of G56.0 documented in the notes. |
Ensuring Clean Claim Submissions
To avoid denials during the pre-adjudication review, every ICD 10 carpal tunnel syndrome code must reflect the "laterality" of the procedure. For example:
- If surgery (CPT 64721) is performed on the right wrist, use 01 and the -RT modifier.
- If surgery is performed on the left wrist, use 02 and the -LT modifier.
- For bilateral procedures, use 03 and the -50 modifier.
Failure to link the diagnosis to the specific side of the body is a leading cause of billing errors.
Did You Know?
Recent industry benchmarks show that 22% of outpatient orthopedic denials are caused by incomplete linkage between the ICD-10 diagnosis and the CPT procedure. Using integrated claim validation ensures these gaps are closed before the claim is even submitted.
How to Structure Documentation to Avoid Denials
Accurate record-keeping is the most important factor in getting claims approved when using the carpal tunnel syndrome ICD 10 code (G56.0). The CMS frequently flags nerve-compression claims for denial, usually because of simple mistakes like missing the "laterality" (which hand is affected) or using vague terms like "hand pain."
To protect your revenue in 2026, every patient note should include three things:
- The Specific Site: Is it the right, left, or both hands?
- Diagnostic Proof: Did an EMG or NCV test confirm the issue?
- The Reasoning: Why is this specific treatment necessary now?
For example, a note stating "Right-hand numbness due to median nerve compression confirmed by EMG" perfectly supports the code G56.01. Payers like Blue Cross Blue Shield and Cigna use automated systems to reject claims that don't reach this level of detail.
2026 Documentation Gap Analysis
| Documentation Gap | Why Denials Occur | Prevention Strategy |
|---|---|---|
| Missing Laterality | Payers reject "unspecified" codes (G56.00) when a specific side isn't named. | Always specify "right," "left," or "bilateral" to meet CMS precision standards. |
| No Diagnostic Evidence | Claims fail audits if EMG or NCV results aren't mentioned. | Reference test results directly: "EMG confirmed left median neuropathy." |
| Vague Terminology | Terms like "wrist discomfort" do not prove medical necessity. | Use "median nerve compression" or "carpal tunnel syndrome" as defined by clinical criteria. |
| Unlinked Procedures | Procedures like surgery (64721) billed without a linked diagnosis will fail. | Ensure the CPT code is electronically linked to the ICD 10 carpal tunnel syndrome code. |
| Missing History | Surgery is often denied if there's no record of previous splinting or therapy. | Include a timeline of conservative care and why it wasn't enough to fix the problem. |
Strengthening Your Audit Trail
By connecting every detail - from the initial nerve test to previous therapy trials - directly to the ICD 10 for carpal tunnel syndrome, you create a claim that flows through the system without manual review. Modern billing workflows now use a three-tier check to verify that the anatomy, the diagnosis, and the procedure all match perfectly before the claim is sent.
Did You Know?
The CMS CERT 2024 report revealed that 38% of denied musculoskeletal claims were rejected simply because they lacked laterality or failed to mention pre-treatment management. These are errors that are 100% preventable with better documentation.
Why Partner with ProMBS for Carpal Tunnel Syndrome Billing?
In the fast-paced world of orthopedics and neurology, even a small documentation gap can lead to significant revenue loss. At ProMBS, our team ensures that every claim using the carpal tunnel syndrome ICD 10 code meets the rigid 2026 standards set by CMS, AHA, and AHIMA.
We specialize in high-precision billing that reduces the stress of audits. By integrating automated validation and continuous staff training, we catch errors before they leave your office.
How We Protect Your Practice
Managing the ICD 10 for carpal tunnel syndrome requires more than just picking a code; it requires a complete compliance strategy. ProMBS provides:
- Laterality Verification: We double-check every claim to ensure the 5th digit (Right, Left, or Bilateral) matches your clinical notes.
- Procedure Linkage: We verify that your CPT codes (like 64721 for surgery) are correctly linked to the specific ICD 10 carpal tunnel syndrome
- Audit-Ready Records: Our feedback loops help your clinical staff document the "medical necessity" and conservative care history that payers demand in 2026.
More Than Just Coding
In a regulatory environment where 38% of musculoskeletal claims are denied due to simple documentation errors, ProMBS offers peace of mind. We don't just process paperwork; we protect your compliance and optimize your reimbursements.
By converting complex nerve-study data into clean, payer-ready claims, we help your practice focus on what matters most: patient care. When precision and performance are non-negotiable, ProMBS is your partner for predictable revenue success.
Frequently Asked Questions
What is the specific ICD-10 code for carpal tunnel syndrome?
The primary code is G56.0. However, 2026 coding standards require a fifth digit for laterality. Use G56.01 for the right hand, G56.02 for the left, and G56.03 for bilateral cases. Specifying the side prevents "unspecified" denials and confirms medical necessity for insurance payers.
Can I use G56.00 for carpal tunnel syndrome?
While G56.00 represents an unspecified side, you should avoid it in 2026. Payers often reject unspecified codes when clinical notes describe a specific hand. Accurate billing requires documenting exactly which wrist is affected to ensure the diagnosis aligns with the treatment or surgical site.
How do I code bilateral carpal tunnel syndrome?
Assign code G56.03 when median nerve compression affects both wrists. This specific carpal tunnel syndrome ICD 10 code justifies the use of bilateral CPT modifiers, such as -50 for surgery. Clear documentation of symptoms in both hands supports this code and ensures full reimbursement for bilateral procedures.
Which CPT codes pair with carpal tunnel ICD-10 codes?
Common pairings include 64721 for surgical release and 95910 for nerve conduction studies. To ensure claim approval, you must link these procedures to the specific ICD 10 for carpal tunnel syndrome that matches the treated side. This linkage proves the procedure was a direct response to the diagnosis.
Why was my carpal tunnel syndrome claim denied?
Most denials stem from missing laterality or a lack of conservative treatment history. Payers require evidence of prior care, like splinting or injections, before approving surgery. Using a precise ICD 10 carpal tunnel syndrome code and documenting the care timeline creates a defensible, audit-proof claim.