Independent cardiovascular practices and hospital-based heart centers face unprecedented economic pressure. Shifting regulatory mandates, aggressive payer exclusion criteria, and the recent structural overhauls of fundamental coding families have turned cardiology revenue cycle management (RCM) into a high-stakes operational minefield.
For many practices, the primary driver of shrinking margins is not declining patient volume, but systemic revenue leakage. This issue stems directly from utilizing generalist medical billing vendors or struggling under the administrative weight of outdated in-house billing models.
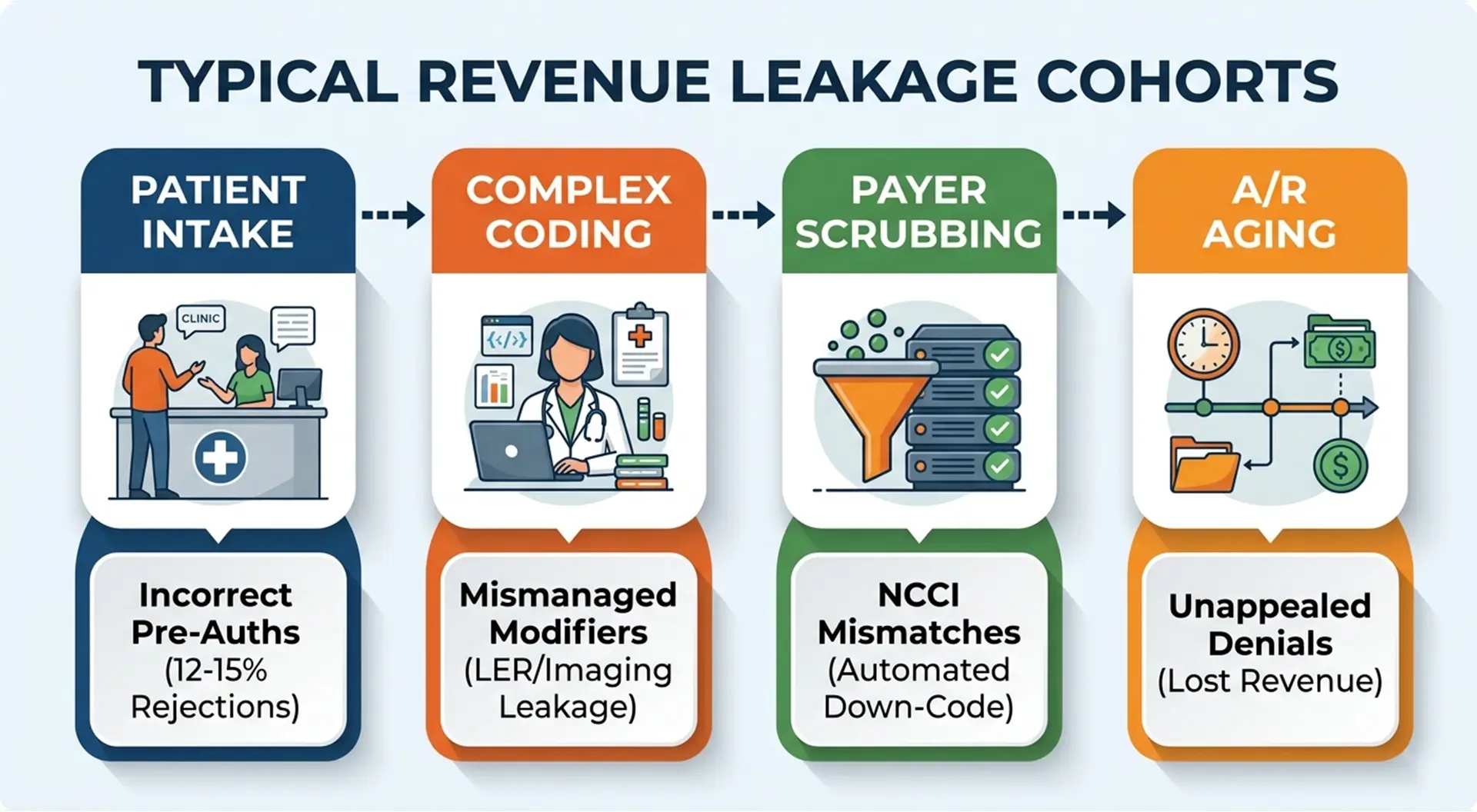
Cardiology is one of the most structurally complex medical fields, spanning routine diagnostic testing, advanced structural imaging, complex electrophysiology (EP), and multi-vessel interventional procedures. A generic approach to medical billing cannot capture these operational nuances.
To maintain financial health, practices require a specialized cardiology medical billing company that deeply understands clinical workflows, compliance guardrails, and payer-specific requirements.
The Anatomy of Cardiology Revenue Cycle Management: Why Generalist Vendors Fail
Generalist billing companies typically process claims across dozens of disparate medical specialties using basic automated code scrubbers. While this model functions adequately for low-complexity, evaluation-and-management (E/M) heavy practices, it fails when applied to the multi-layered rules of cardiovascular billing.
1. The High Cost of “Unbundling” and NCCI Edit Violations
The National Correct Coding Initiative (NCCI) enforces strict code-combination edits designed to prevent “unbundling”—the incorrect practice of billing component parts of a procedure separately when they should be covered under a single comprehensive code. However, generalist providers often make the opposite mistake: they under-bill out of caution, leaving valid revenue unclaimed.
In complex coronary interventions, a single session may include diagnostic cardiac catheterization, fractional flow reserve (FFR) measurement, balloon angioplasty, and multi-vessel drug-eluting stent deployments.
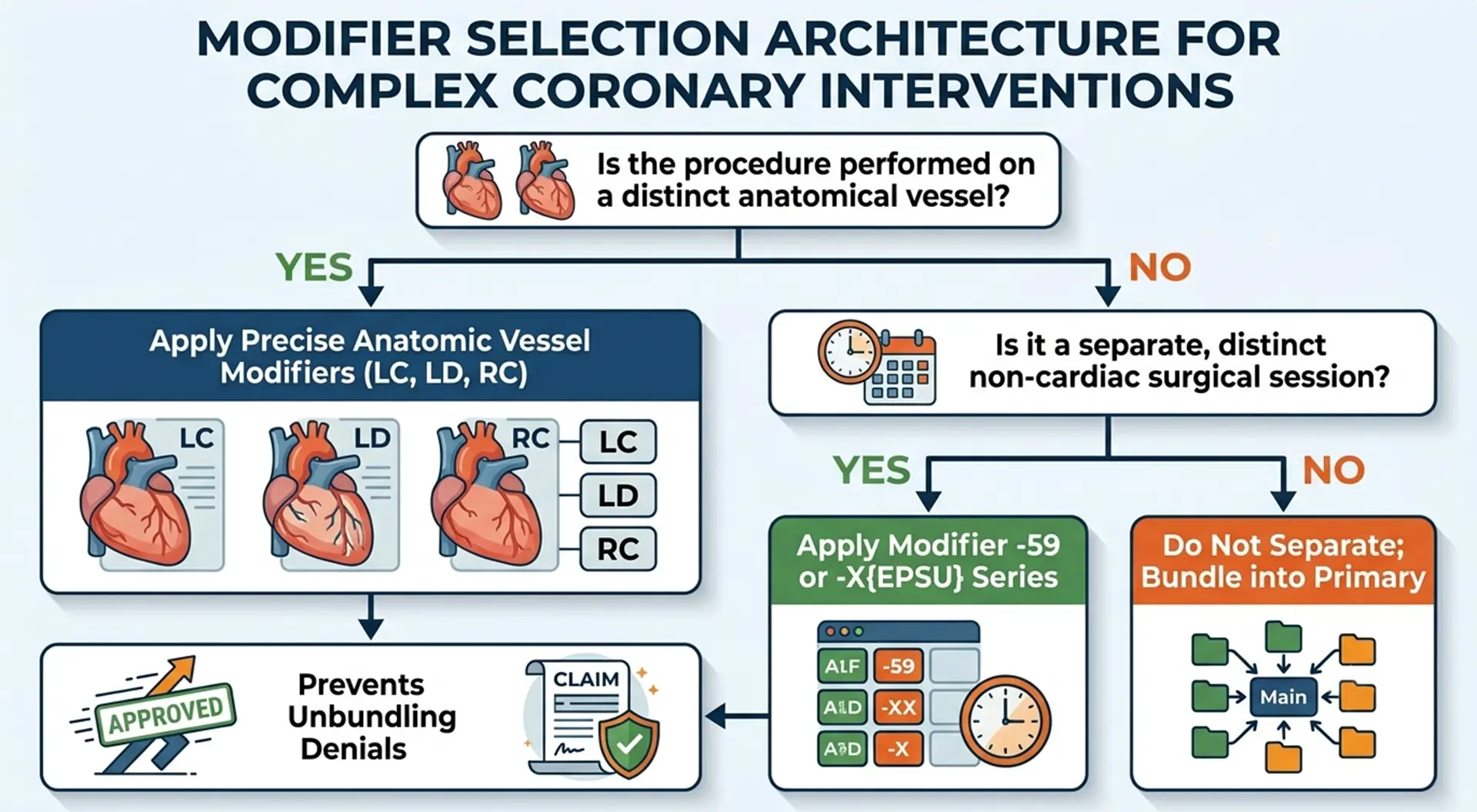
An elite cardiology billing team knows exactly when diagnostic catheterization can be billed separately using Modifier -59 or Modifier -XE. They confirm whether the clinical documentation clearly proves the procedure was a distinct, separately identifiable diagnostic event rather than a routine prerequisite for intervention.
2. Mastering Anatomic and Procedural Modifiers (-25, -59, -X{EPSU})
Modifiers serve as the primary communication mechanism between your practice and payer adjudication engines. Incorrect usage triggers immediate, automated denials, while omission leaves significant money on the table.
-
Modifier -25: This modifier isolates a significant, separately identifiable E/M service performed by the same physician on the same day as a minor procedure (such as an electrocardiogram or echocardiogram). Generalist billers frequently apply Modifier -25 across all visits, triggering automated payer audits. Alternatively, they omit it entirely, losing the professional fee for legitimate consultative care.
-
Modifier -59 and the -X{EPSU} Series: Splitting a global surgical package requires absolute anatomical specificity. Specialist billers utilize the targeted subset modifiers:
-
-XE (Separate Encounter): A service that occurred in a distinct session.
-
-XP (Separate Practitioner): A service distinct because it was performed by a different provider.
-
-XS (Separate Structure): A service performed on a separate anatomical organ or structure (e.g., a distinct coronary artery like the Left Circumflex [LC] versus the Right Coronary Artery [RC]).
-
-XU (Unusual Service): A service that does not typically overlap with the primary procedure.
-
The Modern Cardiology Coding Overhaul: Navigating High-Value Procedure Complexity
The landscape of cardiovascular medicine updates constantly. Specialist billing teams must stay on top of new coding structures to prevent immediate billing rejections.
1. Lower Extremity Revascularization (LER) Coding Protocols
Recent adjustments to the CPT framework completely overhauled the Lower Extremity Revascularization code family (37254–37299). These codes bundle previously separate interventional components—including transcatheter therapies, mechanical atherectomy, and intravascular ultrasound (IVUS)—into highly specific procedural codes.
If your billing company is unaware of these changes, your practice risks severe compliance violations for unbundling components, or significant revenue losses by failing to accurately capture secondary and tertiary vessel treatments.
An elite billing workflow reviews the exact approach (retrograde vs. antegrade), the precise vascular territory (iliac, femoral-popliteal, or tibial-peroneal), and any accompanying mechanical interventions before finalizing the claim submission.
2. Advanced Cardiac Imaging & AI-Based Plaque Quantification
Diagnostic cardiology now relies heavily on advanced imaging modalities. These include Coronary Computed Tomography Angiography (CCTA) paired with AI-driven quantification software.
Coding Case Study: Consider CPT Code 75577 (AI-based quantification of coronary plaque). This code requires explicit documentation of the technical acquisition component alongside the professional interpretive read.
Generalist billing companies often fail to link these services with the appropriate technical capture modifier (0742T), causing payers to reject the entire advanced imaging stack as “not medically necessary.” A specialized team ensures that the machine-generated data logs, software authorization tokens, and clinical interpretations are fully documented within the EHR before submission.
3. Unlocking the Virtual Cardiology Frontier: RPM, RTM, and Telehealth
Remote Patient Monitoring (RPM) and Remote Therapeutic Monitoring (RTM) have expanded the continuity of cardiac care. Managing patients with chronic heart failure or arrhythmias via cellularly connected weight scales, blood pressure cuffs, and continuous ECG patches generates regular, recurring revenue—provided it is billed correctly.
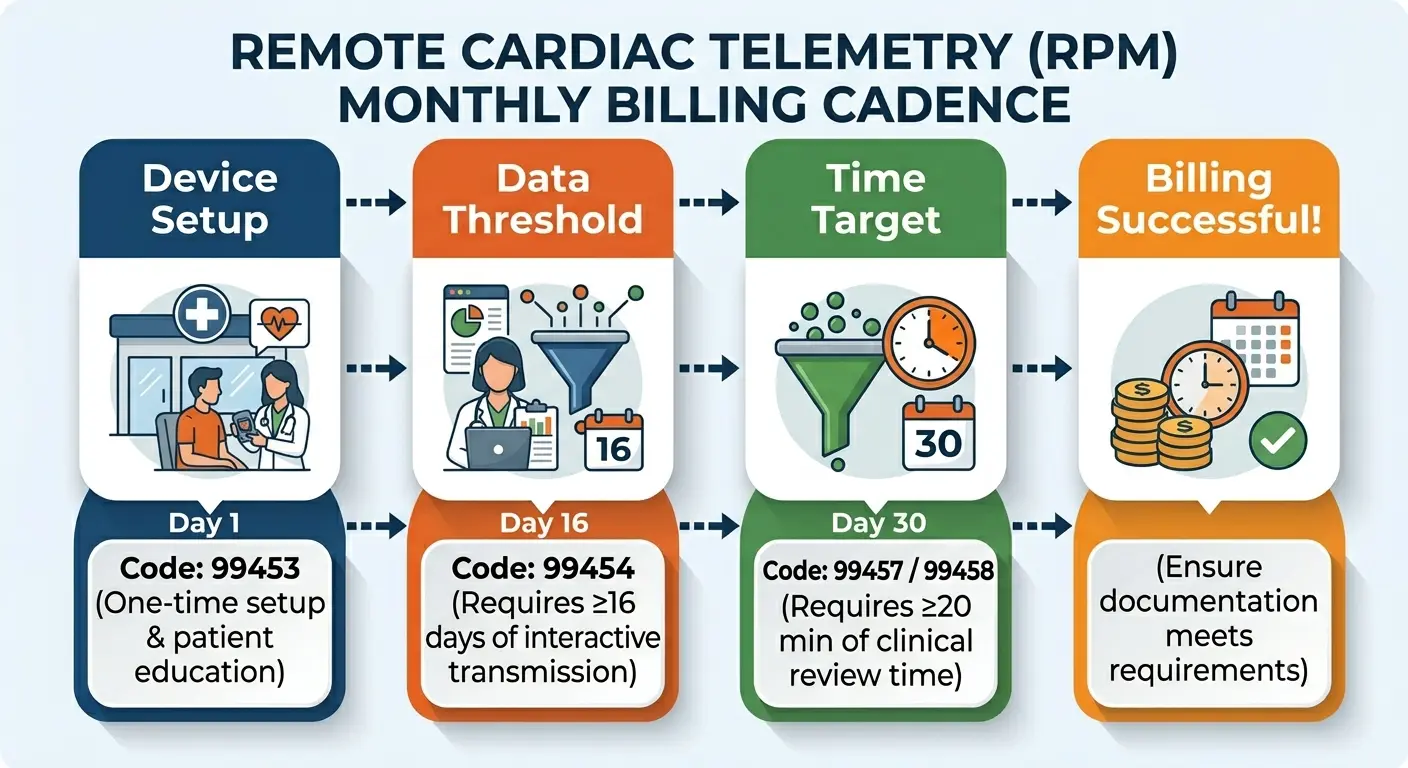
Specialized RCM teams use automated tracking systems to count the exact number of monitoring days each month. This ensures your practice hits the required 16-day transmission minimum for code 99454, while automatically logging the required 20-minute intervals of clinical review time for codes 99457 and 99458.
Performance Benchmarks: Evaluating Elite Cardiology Billing Providers
When assessing independent companies, look closely at their performance metrics. The table below outlines the clear distinctions between average market performance and specialized cardiology RCM standards.
| Financial Performance Metric | In-House Team Average | Generalist RCM Vendor | ProMBS Specialized Standard |
|---|---|---|---|
| First-Pass Clean Claim Rate | 76% – 82% | 84% – 89% | ≥ 98.5% |
| Average Days in A/R (DSO) | 58 – 72 Days | 45 – 55 Days | < 35 Days |
| Net Collection Percentage | 86% – 90% | 89% – 93% | ≥ 97% – 99% |
| A/R Aging Over 90 Days | 22% – 28% | 14% – 18% | < 5% |
| Cardiology Coding Certification | Rare (Generalist CPC) | Generic Offshore Pool | 100% AAPC Certified (CCC) |
| Denial Resolution Cycle | 30 – 45 Days | 21 – 30 Days | < 72 Hours |
Operational Architecture: The End-to-End Specialized Workflow
Achieving an industry-leading clean claim rate requires a structured, multi-phase operational process designed to eliminate errors at every stage of the revenue cycle.
Front-End Intake & Real-Time Eligibility Verification
The workflow begins well before the patient enters the clinic or catheterization lab. Our team uses automated electronic clearinghouses to verify insurance eligibility, determine exact copay/deductible obligations, and confirm active payer enrollment status in real time.
Prior Authorization Mitigation & LCD/NCD Validation
Advanced diagnostic procedures like myocardial perfusion imaging, cardiac MRI, and scheduled angioplasties require strict prior authorization. Our system cross-references the patient’s exact diagnosis codes against active Local Coverage Determinations (LCD) and National Coverage Determinations (NCD) to ensure immediate medical necessity validation.
Certified Clinical Coding & Charge Capture
AAPC-certified Cardiovascular Coders (CCC) review your clinical documentation directly from your EHR (Epic, Cerner, eClinicalWorks). We translate complex procedural notes into precise CPT, ICD-10-CM, and HCPCS code combinations, applying all required anatomical and procedural modifiers.
Predictive Denial Code Scrubbing & Submission
Before submission, every claim passes through a predictive scrubbing engine updated daily with the latest NCCI edits and payer-specific rules. This step catches structural errors, missing modifiers, or invalid code pairings, ensuring a clean submission.
Aggressive Denial Management & Rapid Appeals Tracking
If a payer issues a denial, our specialized denial management team reviews it within 24 to 72 hours. We identify the root cause, reconstruct the clinical appeal package with necessary documentation, and track the claim until payment is successfully recovered.
The Financial Impact: Protecting MIPS Scores and Maximizing Payer Contracts
A premier cardiology medical billing company provides value that goes far beyond processing claims. True partners actively protect your practice’s market standing and improve your bottom line.
Merit-Based Incentive Payment System (MIPS) Optimization
Under the Medicare Access and CHIP Reauthorization Act (MACRA), your practice’s annual Medicare reimbursements are adjusted up or down based on your reported MIPS performance score. Generalist billers often default to low-value, basic quality measures that fail to demonstrate the high quality of your specialized care.
An expert cardiology RCM provider guides your team to select high-priority specialty measures, such as Acute Cardiovascular-Related Hospital Admission Rates or Avoidance of Unnecessary Advanced Imaging. Maximizing these performance categories protects your practice from penalties and helps you secure positive payment adjustments from CMS.
Data-Driven Payer Contract Negotiations
Commercial fee schedules are rarely fixed. However, to negotiate better rates with major insurers, your practice needs clear, organized data on your historical utilization patterns, patient risk profiles, and clean-claim performance metrics.
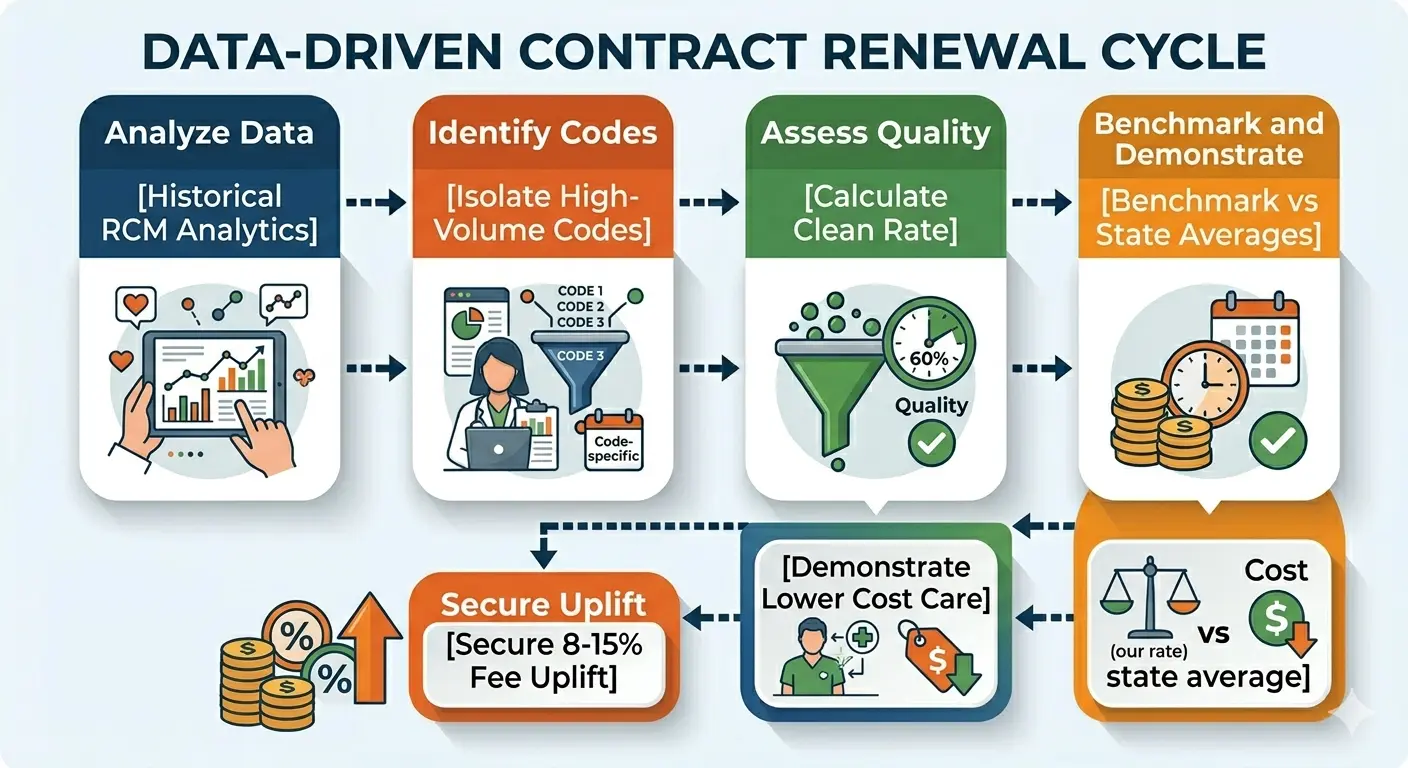
A specialized billing partner provides clear, real-time financial reporting that isolates your highest-volume CPT codes. Armed with this regional cost and performance data, your practice can negotiate favorable commercial fee schedules, often resulting in an immediate 8% to 15% increase in contract rates.
Comprehensive Cardiology Billing FAQ Section
How do you prevent denials for “lack of medical necessity” on advanced cardiac stress tests?
We prevent these denials by using a proactive front-end cross-reference engine. Before a claim for an advanced diagnostic procedure (such as a nuclear stress test) is submitted, our team confirms that the patient’s chart contains clear documentation of supporting symptoms, such as atypical chest pain, ischemia, or pre-existing coronary artery disease, matching active regional LCD guidelines.
What is your process for integrating with our existing cardiology-specific EHR system?
Our billing platform connects with your current system using native HL7 and FHIR interoperability standards. Whether your practice runs on Epic, Cerner, Allscripts, or eClinicalWorks, we establish a secure data bridge that transfers clinical notes and demographic records automatically. This eliminates manual data entry errors and ensures an efficient transition with zero operational downtime.
How does your team handle unlisted or highly complex structural heart codes?
When billing for complex structural procedures that lack a standard CPT code, our certified coders build a detailed reference package. This includes the complete operative report, an expert clinical summary explaining the case’s complexity, and a clear comparison to an existing high-value code to justify the requested reimbursement. This thorough approach prevents automated rejections and secures fair payment for complex interventions.
