You’ve just started accepting Medicaid patients. Your first batch of claims goes out. Two weeks later, half of them come back denied — wrong codes, missing authorizations, eligibility issues. Sound familiar?
Medicaid billing trips up even experienced providers. It’s not like commercial insurance. The rules shift by state, reimbursement rates vary, and a single documentation gap can cost your practice thousands in delayed revenue.
Here’s what you need to know upfront: Medicaid now covers more than 80 million Americans, making it the single largest health insurance program in the country, according to CMS 2025 enrollment data. If you’re a provider who wants a piece of that patient population, learning how to bill Medicaid as a provider correctly isn’t optional — it’s essential.
This guide walks you through every step, from enrolling as a Medicaid provider to appealing denied claims. Whether you’re just starting or cleaning up a billing workflow that isn’t working, you’ll find clear, actionable answers here. No jargon. No fluff. Just the process, explained right.
What Is Medicaid and How Is It Different from Medicare?
Medicaid is a joint federal-state health insurance program designed to cover low-income individuals and families, including children, pregnant women, seniors, and people with disabilities. The federal government sets baseline rules, but each state runs its own program — which means billing rules, covered services, and reimbursement rates are different depending on where you practice.
This is one of the most important things new providers miss. What works in Texas won’t automatically apply in California or Florida.
- Texas Medicaid (administered by HHSC) uses a mix of managed care organizations and fee-for-service plans, with heavy reliance on MCOs like Molina and UnitedHealthcare Community Plan.
- California’s Medi-Cal has undergone major transformation under CalAIM, shifting toward community-based care and whole-person health models.
- Florida Medicaid is almost entirely managed care, with regional plans handling most enrollees.
Here’s a quick side-by-side comparison that clears up the confusion between Medicaid and Medicare:
| Feature | Medicaid | Medicare |
|---|---|---|
| Who it covers | Low-income individuals & families | Adults 65+ and people with disabilities |
| Funding source | Federal + State (shared) | Federal only |
| Administration | State-run, state rules | Federally run, national rules |
| Billing form | CMS-1500 or UB-04 (varies by provider type) | CMS-1500 or UB-04 |
| Reimbursement rates | Lower than Medicare; varies by state | Fixed national fee schedule |
| Eligibility changes | Monthly; verify before every visit | Stable; annual re-enrollment |
Keep in mind: some patients qualify for both programs. They’re called “dual eligibles,” and billing them correctly requires understanding how Medicare pays first and Medicaid covers the remainder.
Who Qualifies as a Medicaid Provider?
Not every healthcare professional can automatically bill Medicaid. You have to be actively enrolled and approved by your state’s Medicaid agency before a single claim can be submitted.
Medicaid billing requirements apply to a wide range of provider types, including:
- Physicians (MDs, DOs) — primary care and specialists
- Nurse Practitioners (NPs) and Physician Assistants (PAs)
- Mental and behavioral health providers — licensed therapists (LCSWs, LPCs), psychologists, psychiatrists
- Hospitals — inpatient, outpatient, and emergency departments
- Home health agencies — skilled nursing, physical therapy, aide services
- Federally Qualified Health Centers (FQHCs) — community health centers with special billing rules
- Dental providers — particularly for pediatric Medicaid beneficiaries
- DME (Durable Medical Equipment) suppliers
- Substance use disorder treatment facilities
Each state maintains its own approved provider list, and some states require additional certifications depending on the service type. If you’re a behavioral health provider in New York, for instance, you may need OMH or OASAS credentials on top of your standard medical license.
Bottom line:
Check your state Medicaid agency’s website first, confirm your provider type is eligible, and then begin the enrollment process described in Step 1 below.
How to Bill Medicaid as a Provider?
Here are the eight steps that make up the Medicaid billing process — in the exact order you need to follow them.
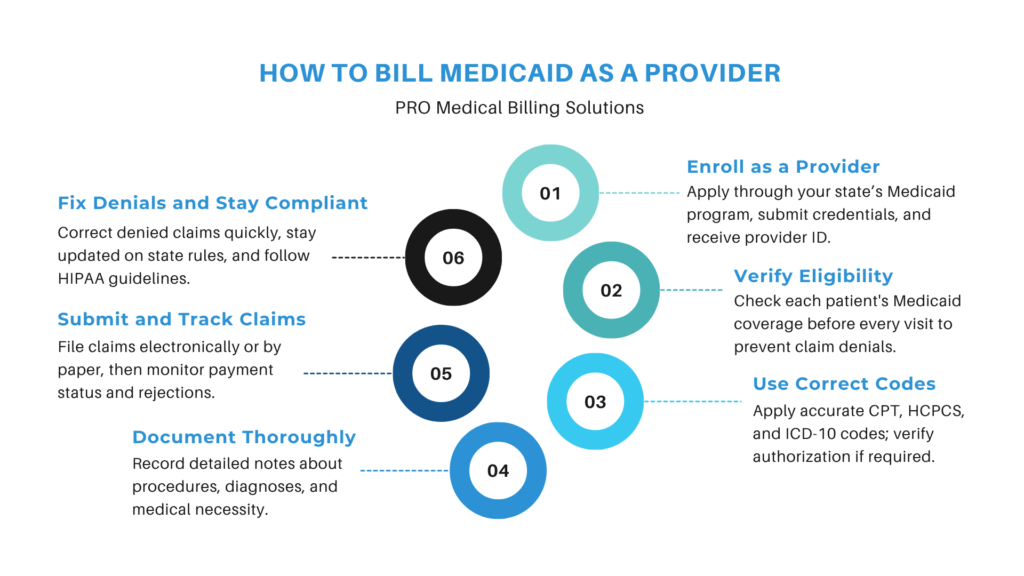
Step 1: Enroll and Credential as a Medicaid Provider
Before you can submit a single claim, you need an approved Medicaid provider number from your state. This is not the same as having an NPI — it’s a separate enrollment with the state Medicaid agency.
If you are new to the process, professional help through Medicaid credentialing services can significantly reduce delays and errors during enrollment.
Documents you’ll typically need:
- National Provider Identifier (NPI) — both Individual (Type 1) and Organizational (Type 2) if billing under a group
- State medical license — must be active and in good standing
- Federal Tax Identification Number (TIN/EIN)
- DEA number — required for prescribing providers
- Proof of malpractice insurance
- CAQH profile — many states use this for credentialing verification
- Practice location information — physical address, contact details
Timeline: Plan for 30 to 90 days from application submission to approval, sometimes longer in states with high application volume. Start this process well before you plan to see Medicaid patients.
Revalidation: Medicaid enrollment isn’t permanent. CMS requires providers to revalidate every 3 to 5 years, and your state may require updates any time your license, address, or ownership information changes. Missing a revalidation deadline can result in your claims being denied or your enrollment being deactivated.
Pro tip:
Some states have separate enrollment processes for managed care organizations (MCOs). If your state uses MCOs, you may need to enroll with each MCO separately in addition to the state fee-for-service program.
Step 2: Verify Patient Medicaid Eligibility Before Every Visit
This step saves more denials than almost anything else in the billing process. Medicaid eligibility changes every single month. A patient who had valid coverage last Tuesday may not have it this Tuesday — income changes, missed renewals, and state eligibility reviews can all affect coverage status.
Never assume. Always verify.
How to check Medicaid eligibility:
- State Medicaid provider portal — most states offer a real-time eligibility lookup tool
- Clearinghouse (e.g., Availity, Change Healthcare) — lets you batch-check multiple patients at once
- Your EHR system — many platforms have built-in eligibility verification through payer connections
MCO vs. Fee-for-Service: Find out whether your patient is enrolled in a Medicaid managed care plan or the state’s traditional fee-for-service program. This matters a lot — if your patient is in an MCO, you’ll bill the MCO directly (not the state), and you’ll follow that plan’s specific rules for prior authorizations, referrals, and covered services.
What to do if a patient isn’t eligible:
Let the patient know before the visit if possible. Offer to reschedule once coverage is confirmed, or discuss self-pay options. Providing services and then discovering coverage lapsed puts you in a difficult collection situation. If the visit already happened, check whether your state allows retroactive eligibility or whether a secondary payer may apply.
Step 3: Obtain Prior Authorization When Required
Skipping prior authorization (PA) is one of the fastest ways to generate an unpayable claim. If a service requires PA and you don’t get it, Medicaid simply won’t reimburse you — and retroactive authorization is not guaranteed.
Many providers streamline this process using prior authorization services to avoid delays and reduce claim denials.
Services that commonly require prior authorization in Medicaid:
- Elective surgeries and procedures
- Specialist referrals (varies by state and plan)
- Durable medical equipment (DME)
- Inpatient hospital admissions (non-emergency)
- Behavioral health services beyond a certain number of visits
- High-cost medications or specialty drugs
- Home health services and skilled nursing facility stays
How to submit a PA request: Most states offer an online portal for PA submissions. You’ll typically need to provide the patient’s Medicaid ID, the service or procedure code, the clinical diagnosis, and supporting documentation showing medical necessity. Some MCOs accept PA requests via fax or phone.
What happens if you skip this step?
Your claim will be denied with a “prior authorization required” or “service not covered without authorization” reason code. You can attempt a retroactive authorization appeal, but these are not guaranteed to be approved and require significant documentation. It’s far easier to get the PA upfront
Step 4: Use Correct Medical Codes (CPT, HCPCS, ICD-10)
Accurate coding is the backbone of a clean Medicaid claim. Use the wrong code — or the right code with the wrong modifier — and your claim will either be denied or, worse, flagged for a compliance audit.
There are three code sets you need to understand:
| Code Type | Purpose | Example |
|---|---|---|
| CPT | Procedure performed | 99213 – Established patient office visit (level 3) |
| ICD-10 | Diagnosis justifying the service | J06.9 – Acute upper respiratory infection, unspecified |
| HCPCS | Equipment, drugs, supplies, non-physician services | A4253 – Blood glucose test strip |
Modifiers matter. Modifiers are two-character additions to CPT or HCPCS codes that provide extra context about how or where a service was delivered. For example:
- Modifier 25 — Significant, separately identifiable E&M service on the same day as a procedure
- Modifier 59 — Distinct procedural service (critical for avoiding bundling denials)
- Modifier GT — Services delivered via interactive audio and video telehealth
Leaving off a required modifier is one of the top five reasons Medicaid claims get denied.
Place of Service (POS) codes are equally important. A service billed with POS 11 (office) instead of POS 02 (telehealth) will be processed differently and may be denied if the documentation doesn’t match the setting.
Always cross-reference your state’s Medicaid fee schedule before billing. Not every CPT code is reimbursable in every state, and some codes have unit limits or age restrictions.
Free Audit
Tired of Medicaid claims coming back denied?
Get a free billing audit and find out exactly where your practice is losing revenue. Response guaranteed within 48 hours.
Claim Your Free Audit ↗
No commitment · 100% free
Step 5: Document Services Thoroughly
Your documentation isn’t just a clinical record — it’s your legal defense in an audit. Medicaid audits are real, and when an auditor reviews your claims, they’re looking to match what you billed to what your notes actually support.
Every clinical note should include:
- Chief complaint — why the patient came in
- History of present illness (HPI) — details about the presenting condition
- Relevant medical and medication history
- Physical examination findings — appropriate to the level of service billed
- Assessment and diagnosis — including the ICD-10 code justification
- Plan of care — treatments, prescriptions, referrals, follow-up
- Time — if billing based on time (certain E&M codes, therapy services)
Many providers use the SOAP note format (Subjective, Objective, Assessment, Plan) as a simple structure to make sure nothing is missed. Whatever format you use, the documentation should clearly justify the service level billed.
If you’re billing a 99214 (moderate complexity E&M), your note needs to reflect moderate complexity — detailed history, multiple diagnoses, prescription management. A note that documents a simple, single-problem visit won’t support that billing level.
Good documentation also matters when submitting PA requests and responding to claim denials. Auditors and reviewers are looking for medical necessity — your notes need to make that case clearly and compellingly.
Step 6: Submit Medicaid Claims Electronically
Once your documentation is complete and your codes are verified, it’s time to submit the claim. Most states strongly prefer — and some require — electronic claim submission.
Which form to use:
| Claim Form | Used By |
|---|---|
| CMS-1500 | Physicians, NPs, PAs, therapists, outpatient providers |
| UB-04 | Hospitals, skilled nursing facilities, home health agencies, ASCs |
How to submit:
- EHR or Practice Management System — most modern EHRs have built-in claim submission through a clearinghouse connection
- Third-party clearinghouse (e.g., Availity, Waystar, Change Healthcare) — validates claims before submission and flags common errors
- State Medicaid provider portal — direct submission option for providers who don’t use a clearinghouse
Timely filing limits: This is critical. Medicaid has strict deadlines for claim submission, and missing them means the claim cannot be paid — period. Timely filing windows vary significantly by state:
- Most states: 90 to 180 days from the date of service
- Some states (including Texas and California) allow up to 365 days
- MCO plans often have their own separate timely filing rules, sometimes shorter than the state’s
Five common errors that get Medicaid claims rejected:
- Wrong or missing NPI — the NPI on the claim must match the enrolled provider exactly
- Incorrect patient Medicaid ID — a single-digit error causes an instant rejection
- Missing or invalid diagnosis code — ICD-10 codes must be at the highest level of specificity
- Unbundled codes — billing separately for services that should be combined under one code
- Date of service doesn’t match authorization — if PA was issued for a different date, the claim won’t process
Step 7: Track Claim Status and Review Remittance Advice
Submitting the claim is not the finish line. You need to actively track every claim through to payment or denial.
How to track claim status:
Most state Medicaid agencies provide a web-based provider portal where you can check the status of submitted claims in real time. Your clearinghouse will also send acknowledgment reports (277CA files) confirming whether claims were accepted or rejected at the payer level.
Electronic Remittance Advice (ERA): When Medicaid processes a claim — paid, adjusted, or denied — they send back an ERA (also called an 835 file). This document tells you exactly what was paid, what was adjusted, and why. Most billing systems can receive and automatically post ERAs.
How to read an EOB and reason codes: The Explanation of Benefits (EOB) includes adjustment reason codes (CARCs) and remittance advice remark codes (RARCs). For example:
- CO-4 — The procedure code is inconsistent with the modifier used
- CO-97 — The benefit for this service is included in the payment for another service
- PR-96 — Non-covered charge
Understanding these codes quickly tells you whether a claim needs to be corrected and resubmitted, appealed, or written off. Build a working knowledge of the most common codes you see in your practice — it dramatically speeds up your denial resolution workflow.
Step 8: Handle Denied Claims and File Appeals
Denials are not the end of the road — they’re a detour. Most denied Medicaid claims can be recovered if you act quickly and correctly.
Top 5 Medicaid denial reasons and how to fix them:
| Denial Reason | Fix |
|---|---|
| Incorrect or missing NPI | Verify the NPI on the claim matches your enrollment record; resubmit with corrected NPI |
| Eligibility issue (coverage not active) | Re-verify eligibility on the exact date of service; check for retroactive coverage or dual eligibility |
| Missing modifier | Identify the required modifier from your state’s fee schedule and resubmit with the correct modifier |
| Prior authorization missing or expired | Request retro-authorization or file an appeal with clinical documentation proving medical necessity |
| Timely filing exceeded | Submit an appeal with proof of timely filing — clearinghouse submission reports, EDI acknowledgment files, or system timestamps |
The appeals process: When you file an appeal, include the original claim, the denial explanation, the corrected or additional documentation, and a written statement explaining why the claim should be paid. Most states require appeals to be filed within 30 to 120 days of the denial date, depending on the state and plan.
For complex denials involving medical necessity, consider attaching clinical literature, peer-reviewed guidelines, or a physician attestation letter. Managed care plans in particular respond well to well-documented clinical appeals.
Track your appeals the same way you track claims — follow up if you haven’t received a response within the payer’s stated turnaround time.
PROVEN RESULTS
Stop leaving Medicaid revenue on the table.
Pro-MBS helps providers cut denial rates, fix coding errors, and recover every dollar they’ve earned. Let’s talk about your practice.
Multi-state coverage · All provider types
Medicaid Billing for Specific Provider Types
Even experienced billing teams make these errors. Here’s what to watch out for — and what each mistake actually costs you.
- Upcoding services. Billing a 99215 when the documentation only supports a 99213 is a compliance violation. CMS has increased its post-payment audit activity in 2025–2026, and upcoding is a top trigger for RAC and PERM audit scrutiny.
- Unbundling codes. Submitting multiple CPT codes for services that should be billed under a single comprehensive code. For example, billing a wound closure and the E&M separately when the E&M is included in the global surgical package.
- Skipping prior authorization. We covered this earlier, but it’s worth repeating — it’s among the top three reasons claims are denied with no path to recovery.
- Using the wrong Place of Service (POS) code. Billing telehealth visits with POS 11 (office) instead of POS 02 (telehealth) creates a documentation mismatch that can trigger a compliance review.
- Not checking state fee schedule updates. Medicaid fee schedules are updated periodically — sometimes annually, sometimes mid-year. If you’re billing codes at rates that were adjusted months ago, you may be leaving money on the table or billing incorrectly.
- Billing without a current provider enrollment. If your enrollment has lapsed due to a missed revalidation or license update, every claim you submit will be denied. Always keep your enrollment record current.
- Ignoring MCO-specific rules. If your patient is in a managed care plan, that plan’s rules govern — not just the state’s. Different MCOs have different PA requirements, timely filing windows, and preferred submission methods. Treating every Medicaid claim the same is a recipe for denials.
Pro-MBS specializes in Medicaid billing for a wide range of provider types across multiple states. From enrollment and credentialing to denial management and appeals, Pro-MBS handles every step of the Medicaid billing process so you don’t have to.
Frequently Asked Questions
Q1: How long does it take to get paid from Medicaid?
Most state Medicaid programs process clean electronic claims within 14 to 30 days of submission. Paper claims take longer, typically 30 to 45 days. Managed care organizations may have slightly different timelines depending on their internal processing cycles. Delays usually indicate a claim is pending review or has been flagged for additional documentation.
Q2: Can I bill Medicaid and Medicare at the same time?
Yes — patients who qualify for both programs are called “dual eligibles.” In most cases, Medicare is billed first as the primary payer. Medicaid then acts as a secondary payer, covering cost-sharing amounts like deductibles and copays that Medicare doesn’t cover. Each claim must be submitted correctly to both programs, and coordination-of-benefits rules apply.
Q3: What is the timely filing limit for Medicaid claims?
Timely filing limits vary by state and by plan type. Most states set the window at 90 to 365 days from the date of service. Managed care plans often have shorter windows — sometimes as few as 90 days. Always check your state Medicaid agency’s billing manual and any MCO provider agreements for the exact limits that apply to your practice.
Q4: What happens if Medicaid denies my claim?
A denial isn’t final. You can correct and resubmit the claim if the denial was due to a fixable error (wrong code, missing modifier, etc.), or file a formal appeal if the denial was based on medical necessity or authorization issues. Most states allow 30 to 120 days to file an appeal. Act quickly — the sooner you respond, the better your recovery rate.
Q5: Do I need a separate NPI for Medicaid billing?
You don’t need a new NPI — your existing Type 1 (individual) and Type 2 (organizational) NPIs are used for Medicaid. However, you do need to make sure both NPIs are linked correctly in your Medicaid enrollment record. Many denials happen because the billing NPI doesn’t match the rendering provider’s NPI or the group’s enrollment data. Review your enrollment file carefully.
Q6: How often does Medicaid update its billing codes and fee schedules?
Most state Medicaid programs update their fee schedules annually, often effective January 1st of each year. Some states issue mid-year updates for specific service categories. CMS also releases annual CPT code updates (effective each January) and ICD-10 updates (effective each October). Staying on top of these changes is essential — billing discontinued codes or outdated rates can lead to denials or compliance issues.
Final Thoughts
Mastering how to bill Medicaid as a provider comes down to eight key steps: enroll correctly, verify eligibility before every visit, get prior authorizations, use accurate codes, document thoroughly, submit clean claims on time, track payments, and work your denials quickly. Get these right consistently, and your Medicaid revenue cycle will run significantly smoother.
The process gets more manageable with experience and the right systems in place. But you don’t have to figure it all out on your own — and you shouldn’t have to spend hours chasing claims when you could be focusing on your patients.
Want to eliminate Medicaid billing errors and get paid faster? Contact PROMBS today for a free billing audit. Our team of revenue cycle specialists will identify gaps in your current billing workflow, flag compliance risks, and show you exactly where your practice is leaving money on the table.