Obstetrics is the general branch of medicine focused on pregnancy, labor, and postpartum care for women, while perinatal refers to the specific, high-risk subspecialty (often called Maternal-Fetal Medicine or perinatology) that manages complex health complications for both mother and fetus during that time.
Understanding this distinction is the first step toward coding accuracy. In the 2026 guidelines, this differentiation determines which chapter of the ICD-10-CM manual you pull from:
Obstetrics Focus (Chapter 15): Codes from the O00-O9A range are designated for the maternal record. These codes describe the mother’s health, complications of pregnancy, and the management of labor.
Perinatal Focus (Chapter 16): Codes from the P00-P96 range are reserved for the newborn record. These are used for conditions that originate before birth or within the first 28 days of life, even if the condition persists as the child grows.
With the rise of AI-driven medical auditing, payers are now more sensitive to "cross-pollination" errors, where a maternal code is incorrectly applied to a newborn’s claim. For example, if a mother has gestational diabetes, the obstetrics coder uses an 'O' code for her chart.
However, if the infant experiences neonatal hypoglycemia as a result, the coder must use a 'P' code (e.g., P70.0) on the infant's chart to ensure the claim is valid and reflects the correct patient.
Key Conditions in Obstetrics & Perinatal Care for 2026
Obstetrics and perinatal conditions encompass a broad spectrum of disorders affecting the mother during pregnancy, delivery, and the puerperium, as well as the fetus or neonate. Accurate documentation is the pivot point for 2026 reimbursement.
Common Maternal Conditions
Gestational Hypertension (O13.-): A pregnancy-induced hypertensive disorder typically developing after 20 weeks. In 2026, coders must specify the trimester (e.g., O13.3 for the third trimester) to ensure medical necessity for increased monitoring.
Gestational Diabetes (O24.4-): This form of glucose intolerance arises during pregnancy. Documentation must specify if it is diet-controlled (O24.410) or insulin-controlled (O24.414) to prevent claim denials.
Placenta Previa (O44.-): Implantation over the cervical os. For 2026, documentation of hemorrhage (or lack thereof) is required for high-level specificity.
Preeclampsia & Eclampsia (O14.-, O15.-): These are systemic hypertensive emergencies. Eclampsia (seizures) is an obstetric crisis that requires immediate, high-acuity coding.
Postpartum Hemorrhage (O72.-): Excessive blood loss following delivery. Note that FY 2026 guidelines clarify that O72.1 should not be used for post-abortion conditions.
Common Neonatal Conditions
Neonatal Jaundice (P59.-): Hyperbilirubinemia is often managed with phototherapy. For 2026, use P59.20 for jaundice from unspecified hepatocellular damage.
Neonatal Respiratory Distress (P22.0): Also known as Hyaline Membrane Disease. It is a frequent perinatal diagnosis for premature infants requiring surfactant or ventilation.
Low Birth Weight & Prematurity (P05, P07): Defined as weight below 2,500g. 2026 coding requires specific codes for both birth weight and gestational age to capture the true acuity of the case.
Congenital Infections (P35-P39): Includes conditions like congenital CMV (P35.1) or Sepsis of the newborn (P36.-).
Essential ICD-10-CM Codes for Obstetrics & Perinatal Care (2026)
The 2026 ICD-10-CM updates emphasize the need for granular documentation to support medical necessity. The following table highlights high-volume codes in obstetrics and perinatal health, incorporating the latest FY 2026 guidelines.
| ICD-10-CM Code | Condition | FY 2026 Documentation Requirements |
|---|---|---|
| O14.03 | Mild/Moderate Pre-eclampsia (3rd Trimester) | Must document trimester. For 2026, ensure proteinuria levels are noted to distinguish from gestational hypertension. |
| O36.4XX- | Maternal Care for Intrauterine Death | Documentation must include the specific week of gestation (Z3A) to validate high-risk management. |
| O80 | Normal Delivery | Use only for full-term, uncomplicated singleton deliveries without any "O" codes from other categories. |
| O9A.31- | Physical Abuse Complicating Pregnancy | (2026 New Focus): Sequence first, followed by codes for specific injuries. Reflects the 2026 priority on SDOH and patient safety. |
| P07.3- | Preterm Newborn | Critical for perinatal reporting. Requires documentation of birth weight (P07.0-) to be coded alongside for full acuity. |
| P22.0 | Neonatal Respiratory Distress | Distinguish from transient tachypnea (P22.1). Requires clinical confirmation of lung immaturity or surfactant use. |
| P59.0 | Neonatal Jaundice (Preterm) | Document bilirubin levels and specific treatment (phototherapy) to support medical necessity. |
| P96.1 | Neonatal Withdrawal (Maternal Use) | (2026 Clarification): Differentiates between maternal drug "addiction" vs. "therapeutic use" (use P96.2 for therapeutic). |
Why Are These Codes Important for Billing?
Correct application of obstetrics and perinatal ICD-10-CM codes is critical for substantiating medical necessity in maternal and fetal monitoring, diagnostic imaging, delivery procedures, and neonatal interventions. In the 2026 reimbursement landscape, precise alignment with CPT® procedure codes is the only way to facilitate clean claim submission and optimize first-pass approval rates.
Inaccurate, nonspecific, or incomplete coding, such as failing to document the exact trimester or birth weight, increases the risk of claim denials, revenue leakage, and payer audits.
Did You Know?
According to the FY 2025 CMS Improper Payments Report, the Medicare Fee-for-Service error rate was 6.55%, while the Medicaid error rate was 6.12%. A staggering 77% of these Medicaid errors were attributed to insufficient documentation. By mastering the 2026 obstetrics and perinatal updates, providers can directly combat these trends, ensuring precise code selection that maintains a steady and compliant revenue flow.
When and How to Apply ICD-10 Obstetrics & Perinatal Codes in 2026
Timing and sequencing are the most scrutinized elements of an audit. In the 2026 fiscal year, automated payer systems are increasingly using AI to flag "nonspecific" sequencing.
When to Use These Codes as Primary Diagnoses:
Obstetrics Focus: The patient encounter is directly related to pregnancy management, labor, or postpartum complications.
Perinatal Focus: The neonate requires intervention for a condition originating in utero or within the first 28 days of life.
Primary Sequencing: When no other secondary diagnosis more accurately explains the immediate clinical picture (e.g., using O13 for a pregnancy-induced hypertension visit).
When to Avoid These Codes:
Underlying Conditions: If a complication is clearly due to a pre-existing medical condition that is not aggravated by the pregnancy (though most pre-existing conditions are coded from Chapter 15 during pregnancy).
Vague Documentation: If the clinical record lacks confirmation, such as "suspected" fetal growth without ultrasound evidence.
2026 Reference: Related Diagnosis Codes
These codes represent the standard for precise clinical documentation in the current cycle:
| ICD-10 Code | Description | Clinical Context |
|---|---|---|
| O13.- | Gestational hypertension | Use for hypertension without proteinuria. |
| O24.4- | Gestational diabetes mellitus | Specify if diet or insulin-controlled. |
| O36.5XX- | Maternal care for poor fetal growth | Requires a 7th character for fetus identification. |
| P05.1- | Small for gestational age | Vital for perinatal acuity tracking. |
| P59.9 | Neonatal jaundice, unspecified | Ensure bilirubin levels are documented. |
| P96.1 | Neonatal withdrawal (maternal use) | Updated 2026 guidance for drug exposure. |
CPT® Integration: Substantiating Medical Necessity
Correctly pairing obstetrics and perinatal ICD-10 codes with CPT® procedure codes is the only way to safeguard your revenue cycle from "Medical Necessity" denials.
| CPT® Code | Description | Typical Linked ICD-10 |
|---|---|---|
| 59400 | Routine obstetric care (Vaginal) | O80 (Normal delivery) |
| 59510 | Cesarean delivery | O34.211 (Scar from previous C-section) |
| 59610 | VBAC delivery | O66.41 (Failed trial of labor) |
| 99460 | Initial hospital care for newborn | Z38.00 (Single live birth) |
| 99464 | Attendance at delivery | P07.3 (Preterm newborn) |
By ensuring these codes align, you demonstrate to payers that the procedure was a direct response to a documented diagnosis. This precise linkage reduces audit exposure and supports consistent revenue integrity across all maternal and neonatal encounters.
Common Causes of Claim Denials in 2026
In the current obstetrics and perinatal billing environment, claim denials are increasingly triggered by automated AI-scrubbers used by payers. Understanding these triggers is essential for maintaining revenue integrity.
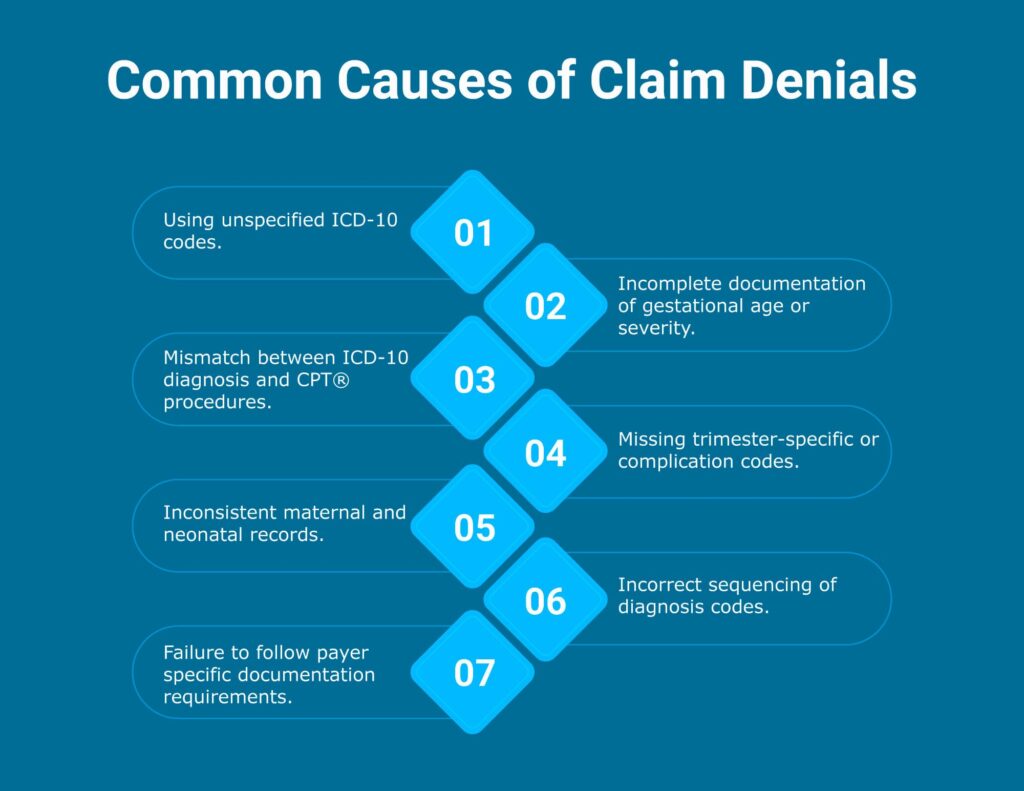
Top 7 Denial Triggers to Avoid:
Overuse of Unspecified Codes: Utilizing unspecified ICD-10-CM codes when more specific trimester- or condition-based codes are available. In 2026, many payers have implemented hard stops for "Unspecified" codes in Chapter 15.
Documentation Gaps: Incomplete clinical notes regarding gestational age, severity of the condition, onset, or specific maternal/fetal outcomes.
Diagnosis-Procedure Mismatch: A discrepancy between the ICD-10-CM diagnosis codes and the CPT® procedure codes. For example, billing for a high-risk delivery (CPT 59510) without a supporting high-risk diagnosis like O14.03.
Trimester Omissions: Failing to include trimester-specific codes (e.g., 1st, 2nd, 3rd trimester), which are required for accurate medical necessity validation.
Record Inconsistency: Conflicts between the maternal record and the neonatal record. Payers often flag cases where a perinatal complication is noted on the baby's claim but has no corresponding "affected by maternal condition" code.
Sequencing Errors: Improperly assigning codes, such as failing to place the obstetrics condition as the primary diagnosis during an antepartum encounter.
Payer-Specific Non-Adherence: Ignoring unique documentation requirements set by private payers or state Medicaid programs regarding perinatal risk assessments.
Strategic Action Plan: How to Outsmart 2026 Billing Denials
While identifying triggers is the first step, a proactive approach is required to safeguard your obstetrics and perinatal revenue. Use these three pillars of "Prevention-First" billing:
Clinical Substantiation: Don't just list codes; ensure your clinical notes explicitly document the "Why." For 2026, payers require a clear link between gestational age and maternal/fetal outcomes to validate the medical necessity of high-frequency monitoring.
The "Chart Separation" Rule: Maintain a strict firewall between maternal and infant records. Apply P-codes exclusively to the newborn’s chart. Misplacing a 'P' code on a maternal chart is a leading cause of "Discrepancy Denials" in automated payer systems.
Pre-Submission Quality Checks: Implement a "Claim Scrubbing" workflow that catches sequencing errors before they leave your desk. Ensuring your obstetrics diagnosis is sequenced as the primary encounter reason is the most effective way to expedite reimbursement and minimize audit exposure.
2026 Documentation Checklist: Obstetric and Perinatal Precision
Comprehensive, high-fidelity documentation is the only way to satisfy 2026's AI-driven payer audits. To ensure your claims are bulletproof, every medical record should include:
Gestational Age and Trimester: Specify the exact gestational week. In 2026, "unspecified trimester" codes are the leading cause of manual medical reviews.
Maternal Complications: Record hypertension (HTN), gestational diabetes (including control methods), and infections. These are critical for risk adjustment and hierarchical condition category (HCC) coding.
Delivery Specifics: Document the method (Vaginal, C-section, or VBAC) and any complications encountered during labor. This ensures alignment between ICD-10 and CPT® codes.
Neonatal Acuity Metrics: Include Apgar scores, prematurity status, and birth weight. These metrics are the primary drivers for perinatal code specificity.
Supporting Clinical Evidence: Capture all pertinent lab results, ultrasound findings, and therapy details to substantiate the medical necessity of the care provided.
Partner with Pro-MBS for Smarter, Compliance-Driven Billing
At ProMBS, we specialize in the unique complexities of obstetrics and high-risk perinatal billing. Our certified specialists act as an extension of your team, ensuring that the 2026 ICD-10-CM updates are seamlessly integrated into your revenue cycle.
We go beyond routine claim processing. By combining advanced billing protocols with proactive denial management, we help you achieve:
- Higher First-Pass Acceptance Rates: Through rigorous documentation integrity audits.
- Faster Reimbursements: By eliminating the sequencing errors and "unspecified" code triggers.
- Sustainable Growth: Allowing you to focus on patient care while we secure your financial health.
Frequently Asked Questions
How does the 2026 ICD-10 update change obstetric billing?
The 2026 guidelines mandate extreme trimester specificity to validate medical necessity. Payers now use automated systems to reject "unspecified" codes. Accurate documentation of the exact week of gestation is the only way to justify high-risk monitoring and ensure your practice receives full reimbursement without manual medical reviews.
Can you use perinatal codes on a maternal medical record?
No, you must never place P-codes on a maternal chart. These codes strictly identify conditions originating in the fetal or neonatal period and belong exclusively to the newborn’s record. Mixing these chapters triggers immediate "mismatch" denials that stall your revenue cycle and complicate audit trails.
What defines the perinatal period for ICD-10-CM coding?
The perinatal period begins before birth and extends through the first 28 days of life. Coding within this range focuses on conditions that originate in utero, even if they persist long-term. Precise documentation of this window ensures you capture the correct acuity level for neonatal claims.
Why is the distinction between obstetrics and perinatology critical?
Obstetrics manages the mother’s health, while perinatology focuses on high-risk fetal and neonatal complications. Distinguishing these specialties in your documentation allows for accurate code sequencing. This clarity prevents payers from downcoding complex maternal-fetal encounters, securing the higher reimbursement rates associated with specialized, high-acuity care.
How do social determinants impact 2026 perinatal outcomes?
The 2026 updates emphasize "Code Also" instructions for social determinants, such as housing or transportation instability. Linking these factors to a perinatal diagnosis provides the clinical context necessary to justify intensive care. This holistic documentation style proves medical necessity to AI-driven insurers, reducing the likelihood of audits.